

💡 What You Need to Know Right Away
A mammogram is a screening test that uses low-dose x-rays to create detailed images of breast tissue, helping doctors detect breast cancer early when treatment is most effective.
Also known as: Mammography, breast imaging, breast x-ray, digital mammography, screening mammogram
- Regular screening helps prevent breast cancer deaths. In women ages 50-59, research shows screening helped prevent about 8 deaths for every 10,000 women screened over 10 years[Evidence: A][1]
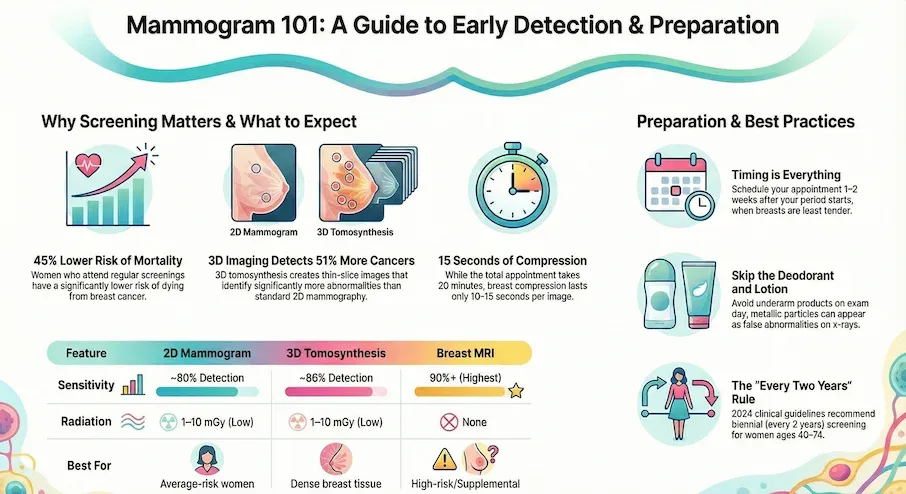
- Women who attend screening regularly have about 45% lower risk of dying from breast cancer compared to non-attendees[Evidence: A][2]
- 3D mammography (tomosynthesis) detects about 51% more cancers than standard 2D mammography[Evidence: B][7]
- The entire procedure takes about 15-20 minutes, with breast compression lasting only 10-15 seconds per image
If you are preparing for your first mammogram or wondering whether it is time to schedule your next one, you are not alone. Many people feel anxious about what the procedure involves, whether it will hurt, and what the results might show.
The good news is that mammograms are one of the most studied and effective tools for detecting breast cancer early. Current clinical guidelines recommend biennial screening starting at age 40 for women at average risk[Evidence: D][15]. This guide explains everything you need to know, from how the test works to what your results mean, so you can approach your appointment with confidence.
❓ Quick Answers
What is a mammogram?
A mammogram is a low-dose x-ray of your breast tissue that creates detailed images doctors use to detect breast cancer, often years before you can feel a lump. Two types exist: screening mammograms for routine checkups in women without symptoms, and diagnostic mammograms for investigating symptoms or abnormal findings.
Is a mammogram painful?
Most women experience moderate discomfort rather than true pain. The compression feels like firm pressure for 10-15 seconds per image. About 30% of women report no pain, 50% report moderate discomfort, and 20% report significant pain. Scheduling 1-2 weeks after your period starts can reduce discomfort since breasts are less tender then.
How often should I get a mammogram?
Clinical guidelines recommend biennial (every 2 years) screening for women ages 40-74[Evidence: D][15]. Research found no difference in detecting advanced cancers between annual and every-two-years screening[Evidence: D][16]. Your doctor may recommend more frequent screening if you have risk factors.
What age should I start getting mammograms?
The U.S. Preventive Services Task Force recommends starting at age 40 with biennial screening[Evidence: D][15]. In women ages 39-49, screening helped prevent about 3 breast cancer deaths for every 10,000 women screened over 10 years[Evidence: A][1].
Is mammogram radiation safe?
Yes. The radiation dose is very low, about 1-10 milligrays per exam[Evidence: C][14]. Research suggests screening radiation may cause fewer than 1.3 additional breast cancers per 100,000 women over a lifetime, a risk considered very low compared to the benefit of detecting existing cancers[Evidence: C][14].
How long does a mammogram take?
The entire appointment takes about 15-20 minutes, including changing clothes and positioning. The actual imaging takes only a few minutes, with each breast compression lasting just 10-15 seconds. You typically receive four images total: two views of each breast.
What is 3D mammography?
3D mammography (digital breast tomosynthesis) creates multiple thin-slice images of your breast that the radiologist can view layer by layer. Research shows 3D mammography correctly identifies cancer in about 86 out of 100 cases compared to about 80 out of 100 with standard 2D[Evidence: A][5].
What should I not wear to a mammogram?
Avoid deodorant, antiperspirant, lotion, or powder on your underarms or breasts. These products contain particles that can appear as white spots on the x-ray and be confused with abnormalities. Wear a two-piece outfit so you only need to remove your top. Leave jewelry at home.
Mammogram Health Guide
Early detection is the most powerful tool in breast health. Understand the process, preparation, and importance of regular screenings through this comprehensive guide.
🔬 How Does Mammography Work?
Think of a mammogram like pressing a book flat to read every page clearly. When your breast tissue is compressed between two plates, the x-ray can see through each layer without overlapping tissue hiding potential problems.
The mammography machine sends a low-dose x-ray beam through your breast tissue. Different types of tissue absorb the radiation differently. Dense fibroglandular tissue (the milk-producing glands and supporting tissue) appears white on the image. Fatty tissue appears darker. Tumors and calcifications often appear as bright white spots because they absorb more radiation.
Standard 2D mammography captures a flat image from top-to-bottom and side-to-side angles. 3D mammography (tomosynthesis) moves in an arc during imaging, creating multiple thin slices, typically 1mm thick. This is similar to how a CT scan works. The radiologist can scroll through these slices to examine each layer of breast tissue separately, making it easier to spot abnormalities that overlapping tissue might otherwise hide.
Research shows that mammography sensitivity varies by breast density. In women with fatty breasts, screening correctly identifies cancer in about 80 out of 100 cases. In women with dense breasts, sensitivity drops to about 67 out of 100[Evidence: C][12]. Dense breast tissue appears white on the x-ray, making tumors (which also appear white) harder to detect, like finding a snowball in a snowstorm.
This is why 3D mammography offers particular benefits for women with dense breasts. Studies suggest 3D mammography combined with 2D imaging detected about 89% of cancers compared to 87% with 2D alone[Evidence: C][6].
🧪 What to Expect: The Real User Experience
During the Procedure
You will undress from the waist up and wear a hospital gown that opens in the front. The technologist will position you standing in front of the mammography machine. Your breast is placed on a flat platform, then a clear plastic plate presses down to flatten the tissue.
The compression feels like a firm, flattening pressure, comparable to a firm handshake applied over a larger area. Each compression lasts only 10-15 seconds while the image is captured. You will need to hold still and briefly hold your breath. The room is typically kept cool (65-68°F) to maintain the equipment, and the plastic plates may feel cold against your skin.
The machine makes a mechanical whirring sound during plate adjustment, but the x-ray capture itself is silent. Unlike an MRI, there is no enclosed space or loud banging. The technologist provides verbal cues throughout: "Hold your breath," "Stay still," "You can breathe now."
What You Will Feel After
About 40% of patients experience mild soreness or tenderness after the procedure, typically resolving within 24 hours. A small percentage (5-10%) report tenderness lasting 48-72 hours. Bruising is rare, occurring in fewer than 5% of cases. You may notice temporary red marks or indentations from the compression plates, which fade within hours.
How to Make It Easier
- Time it right: Schedule 1-2 weeks after your period starts when breasts are least tender
- Pre-medicate: Take ibuprofen or acetaminophen 60 minutes before your appointment
- Breathe deeply: Slow, deep breaths before compression reduces muscle tension
- Speak up: Tell the technologist if pain is severe. They can adjust compression slightly
- Relax your body: Drop your shoulders, relax your arm, avoid tensing chest muscles
- Dress smart: Wear a two-piece outfit so you stay warmer (only remove your top)
- Bring support: Most facilities allow a support person in the waiting room
📊 Preparation and Screening Guidelines
How to Prepare
Proper preparation helps ensure clear images and a more comfortable experience.
| Timing | What to Do | Why It Matters |
|---|---|---|
| 1-2 weeks before | Schedule 1-2 weeks after period starts | Breasts are least tender and swollen |
| Day before | Gather prior mammogram images if from different facility | Radiologist compares current and previous images |
| Day of (morning) | Shower, but skip deodorant, lotion, powder | Products can appear as spots on x-ray |
| 60 minutes before | Take pain reliever if desired | Reduces compression discomfort |
| Before leaving | Wear two-piece outfit, leave jewelry home | Easier changing, no interference with imaging |
Screening Guidelines by Age
Different organizations have slightly different recommendations. The 2024 USPSTF update recommends starting at age 40[Evidence: D][15].
| Age Group | USPSTF 2024 | Deaths Prevented per 10,000 (10 years) | Evidence |
|---|---|---|---|
| 40-49 | Biennial screening recommended | About 3 deaths prevented | [A][1] |
| 50-59 | Biennial screening recommended | About 8 deaths prevented | [A][1] |
| 60-69 | Biennial screening recommended | About 21 deaths prevented | [A][1] |
| 70-74 | Biennial screening recommended | About 13 deaths prevented | [A][1] |
| 75+ | Insufficient evidence (Grade I) | Not established | [D][15] |
Research comparing screening beyond age 74 to stopping at age 74 found no difference in breast cancer deaths[Evidence: D][16]. Discuss with your doctor whether to continue screening after 74 based on your overall health and life expectancy.
⚠️ Risks, Limitations, and What to Know
The mammogram procedure itself is safe and painless for most women. The brief compression may cause temporary discomfort but has no lasting effects. Understanding the limitations of screening helps set realistic expectations.
False Positive Callbacks
It is normal to feel anxious about callbacks. In the United States, about 10 out of 100 women are called back for additional testing[Evidence: C][10]. False positives are more common in women ages 40-49, women with dense breasts (about 64% higher risk), and women getting annual versus biennial screening (more than twice as common)[Evidence: C][9].
Of those called back, only about 4-26 out of 100 actually have cancer, depending on the reason for callback[Evidence: C][10]. Most callbacks result in additional imaging that shows no cancer.
Interval Cancers
In women screened every two years, between about 8 and 21 breast cancers are detected between screening appointments for every 10,000 women screened[Evidence: C][13]. These "interval cancers" tend to be more aggressive and have worse outcomes than cancers detected at routine screening[Evidence: C][13].
Radiation Exposure
The average radiation dose from a mammogram is 1-10 milligrays[Evidence: C][14]. This is roughly equivalent to 2-3 weeks of natural background radiation. Research suggests the lifetime risk of developing cancer from screening radiation is very low compared to the benefit of detecting existing cancers[Evidence: C][14].
🥗 Practical Guidance for Your Mammogram
Day-of Checklist
- Shower in the morning but skip deodorant, lotion, and powder
- Take a pain reliever 60 minutes before if you tend to have breast tenderness
- Bring your insurance card and ID
- Bring prior mammogram images if this is a new facility
- Arrive 15 minutes early to complete paperwork
- Expect the total visit to take 30-45 minutes
After Your Mammogram
Results typically arrive within 3-7 days by mail for routine screening. If an abnormality is detected, you will usually receive a call within 1-2 days. No special care is needed afterward. You can return to all normal activities immediately.
Understanding Your Results Letter
Your results letter will include a BI-RADS category (0-6). Categories 1-2 are normal and require only routine follow-up. Category 0 means additional imaging is needed. Categories 3-6 indicate varying levels of concern, from probably benign to highly suspicious for cancer.
Common Mistakes to Avoid
- Wearing deodorant: Products containing aluminum appear as white spots on x-rays
- Scheduling during your period: Breasts are most tender and swollen, increasing discomfort
- Not mentioning breast changes: Tell the technologist about any lumps, pain, or discharge
- Skipping due to fear: Early detection significantly improves outcomes
What to Look for When Choosing a Mammogram Provider
The quality of your mammogram results depends on the facility and the radiologist interpreting your images. Here's what to consider:
Facility Quality Markers
- FDA certification: All mammography facilities must be FDA-certified under the Mammography Quality Standards Act (MQSA) Why it matters: Federal requirement ensures equipment quality and staff training standards
- ACR accreditation: American College of Radiology accreditation indicates higher quality standards Why it matters: Voluntary accreditation shows commitment to excellence beyond minimum requirements
- 3D mammography availability: Digital breast tomosynthesis detects about 51% more cancers than 2D alone[Evidence: B][7] Why it matters: 3D technology particularly benefits women with dense breasts
- Breast imaging specialists: Dedicated breast radiologists who read hundreds of mammograms Why it matters: Experience improves accuracy and reduces missed cancers
Questions to Ask Before Scheduling
- Do you offer 3D mammography (tomosynthesis)?
- Is the radiologist who will read my images a breast imaging specialist?
- How long until I receive my results?
- What supplemental screening do you offer for dense breasts?
- Is the facility certified by the FDA and accredited by the ACR?
Red Flags
- No FDA certification displayed: All mammography facilities must be FDA-certified
- Only 2D imaging available: 3D mammography is now available at over 90% of US facilities
- Very long wait for results: Results should be available within 30 days by law, but most facilities provide them within 1-2 weeks
- No option for supplemental screening discussion: Women with dense breasts should be informed about additional screening options
How Mammogram Compares to Ultrasound and MRI
Mammography, ultrasound, and MRI each have different strengths for breast cancer detection. Your doctor may recommend additional imaging based on your breast density, risk factors, or mammogram results.
| Feature | Mammogram | Ultrasound | MRI |
|---|---|---|---|
| How It Works | Low-dose x-rays | Sound waves | Magnetic fields and radio waves |
| Radiation Exposure | 1-10 mGy[14] | None | None |
| Sensitivity (2D/3D) | 80-86%[5] | Variable (operator-dependent) | Highest (90%+) |
| Specificity | 96%[5] | Lower (more false positives) | Lower (more false positives) |
| Best For | Routine screening in average-risk women | Evaluating palpable lumps, dense breast supplemental screening | High-risk women, dense breast supplemental screening |
| Procedure Time | 15-20 minutes | 15-30 minutes | 30-60 minutes |
| Cost (Approximate) | $100-300 | $150-500 | $500-3,000 |
When Supplemental Screening May Help
For women with dense breasts, adding MRI to mammography reduced cancers detected between screenings by about 53%[Evidence: D][16]. However, clinical guidelines currently state there is not enough evidence to recommend for or against routine supplemental imaging[Evidence: D][15].
Talk to your doctor about supplemental screening if you have dense breasts (categories C or D on your mammogram report) or other risk factors for breast cancer.
What The Evidence Shows (And Doesn't Show)
What Research Suggests
- Regular mammography screening reduces breast cancer deaths. In women ages 50-59, about 8 deaths were prevented per 10,000 women screened over 10 years[Evidence: A][1]
- Women who attend screening have about 45% lower breast cancer mortality compared to non-attendees, though healthier lifestyles in screeners may partially explain this[Evidence: A][2]
- 3D mammography detects about 51% more cancers than 2D mammography alone, based on over 114,000 women in randomized trials[Evidence: B][7]
- About 22-30% of breast cancer deaths are prevented in women who attend screening regularly at 13-year follow-up[Evidence: A][3]
- Supplemental MRI for women with dense breasts reduces interval cancers by about 53%[Evidence: D][16]
What's NOT Yet Proven
- Optimal screening frequency is not established. Research found no difference in detecting advanced cancers between annual and biennial screening[Evidence: D][16]
- Benefit of screening beyond age 74 is uncertain. No mortality difference was observed when comparing screening versus stopping at age 74[Evidence: D][16]
- Supplemental imaging (ultrasound, MRI) for dense breasts lacks sufficient evidence for routine recommendation[Evidence: D][15]
- Long-term mortality benefit of 3D versus 2D mammography is not established. Most studies show increased cancer detection at first screen, but mortality outcomes require longer follow-up
Where Caution Is Needed
- False positive rates are significant: about 12% per exam, with cumulative 10-year rates of 50-60%[Evidence: C][9]
- Overdiagnosis may affect 19-30% of detected cancers. These are cancers that would never have caused harm during the person's lifetime[Evidence: A][3]
- Dense breasts significantly reduce detection. Sensitivity drops from 80% to 67%[Evidence: C][12]
- Interval cancers (found between screens) tend to be more aggressive with worse outcomes[Evidence: C][13]
Should YOU Get Regular Mammograms?
Best suited for: Women ages 40-74 at average risk for breast cancer. Women with dense breasts should discuss supplemental screening options.
Not recommended for: Women under 40 without high-risk factors. Women with limited life expectancy where screening harms may outweigh benefits.
Realistic timeline: Results typically arrive within 3-7 days for routine screening. Abnormal findings trigger callback within 1-2 days.
When to consult a professional: Before deciding on screening frequency if you have risk factors (family history, BRCA mutations, prior radiation therapy). After any abnormal result. When considering supplemental screening for dense breasts.
Frequently Asked Questions
What does dense breast tissue mean for my mammogram?
Dense breast tissue means you have more fibroglandular tissue (milk glands and supporting tissue) than fatty tissue. About 40% of women have dense breasts. The challenge is that both dense tissue and tumors appear white on mammograms, making cancers harder to spot. Research shows screening sensitivity drops from about 80% in fatty breasts to about 67% in dense breasts. Your mammogram report will include a breast density category (A through D), with C and D indicating dense breasts. If you have dense breasts, discuss supplemental screening options with your doctor.
What do BI-RADS categories mean?
BI-RADS (Breast Imaging Reporting and Data System) is a standardized scoring system radiologists use to describe mammogram findings. Category 0 means additional imaging is needed. Category 1 is negative (no findings). Category 2 is benign (non-cancerous findings noted). Category 3 is probably benign (less than 2% chance of cancer, short-term follow-up recommended). Category 4 is suspicious (biopsy recommended, further divided into 4A, 4B, 4C with increasing suspicion). Category 5 is highly suggestive of malignancy (over 95% likelihood of cancer). Category 6 is known cancer (biopsy-proven).
What is a mammogram callback and should I be worried?
A callback means the radiologist needs additional images to evaluate an area more closely. In the United States, about 10 out of 100 women are called back. It is normal to feel anxious, but most callbacks do not result in a cancer diagnosis. Of women called back, only about 4-26 out of 100 actually have cancer, depending on the finding. Additional imaging usually provides reassurance that the finding is benign.
Can mammograms detect all breast cancers?
No. Mammograms miss some cancers, particularly in women with dense breasts. Research shows that about 20-25 out of 100 cancers found between screening appointments were actually visible on prior mammograms but were missed. 3D mammography improves detection, finding about 51% more cancers than 2D alone. For women at high risk or with dense breasts, supplemental imaging with MRI or ultrasound may be recommended.
What happens after an abnormal mammogram?
If your mammogram shows an abnormality, you will likely be called back for additional imaging, which may include additional mammogram views, ultrasound, or MRI. If the abnormality persists, a biopsy may be recommended. During a biopsy, a small sample of breast tissue is removed and examined under a microscope. Most biopsies show benign (non-cancerous) findings. Your healthcare team will guide you through each step and explain your options.
Do I need supplemental screening if I have dense breasts?
Current clinical guidelines state there is not enough evidence to recommend for or against routine supplemental imaging for women with dense breasts. However, research shows that adding MRI to mammography for women with dense breasts reduced cancers detected between screenings by about 53%. Discuss your individual risk factors with your doctor to determine if supplemental screening is right for you.
What is a false positive mammogram result?
A false positive means the mammogram showed something suspicious that turned out not to be cancer after additional testing. About 12 out of 100 women receive a false positive result on a single screening exam. False positives are more common in younger women, women with dense breasts, and women getting annual screening. While false positives cause anxiety and require additional testing, they are a trade-off for catching real cancers early.
Does Medicare cover mammograms?
Yes. Medicare Part B covers one screening mammogram every 12 months for women age 40 and older with no out-of-pocket cost. Diagnostic mammograms (when investigating symptoms or following up on an abnormal screening) are covered but may involve cost-sharing. Starting in 2026, expanded federal requirements mandate coverage for supplemental screening and patient navigation services for women with dense breasts. Check with your specific Medicare plan for details.
How does AI affect mammogram reading?
Artificial intelligence is being used to assist radiologists in reading mammograms. Research from nearly 90,000 Korean women found that AI correctly identified cancer in about 67 out of 100 cases compared to radiologists who identified 70 out of 100. However, AI correctly ruled out cancer in 93 out of 100 cases without cancer, compared to radiologists at 78 out of 100. AI is currently used to assist, not replace, radiologist interpretation.
Is there a difference between screening and diagnostic mammograms?
Yes. A screening mammogram is a routine exam for women without symptoms, typically involving four standard x-ray images (two of each breast). A diagnostic mammogram is performed when there are symptoms (lump, pain, discharge) or an abnormal finding on a screening mammogram. Diagnostic mammograms include additional images focused on the area of concern and are often combined with ultrasound. The radiologist typically reviews diagnostic mammograms immediately rather than within days.
Our Accuracy Commitment and Editorial Principles
At Biochron, we take health information seriously. Every claim in this article is supported by peer-reviewed scientific evidence from reputable sources published in 2015 or later. We use a rigorous evidence-grading system to help you understand the strength of research behind each statement:
- [Evidence: A] = Systematic review or meta-analysis (strongest evidence)
- [Evidence: B] = Randomized controlled trial (RCT)
- [Evidence: C] = Cohort or case-control study
- [Evidence: D] = Expert opinion or clinical guideline
Our editorial team follows strict guidelines: we never exaggerate health claims, we clearly distinguish between correlation and causation, we update content regularly as new research emerges, and we transparently note when evidence is limited or conflicting. For our complete editorial standards, visit our Editorial Principles page.
This article is for informational purposes only and does not constitute medical advice. Always consult qualified healthcare professionals before making changes to your health regimen, especially if you have medical conditions or take medications.





References
- 1 . Effectiveness of Breast Cancer Screening: Systematic Review and Meta-analysis, Annals of Internal Medicine, 2016, Nelson HD et al. PubMed [Evidence: A]
- 2 . Effect of screening mammography on the risk of breast cancer deaths: a systematic review with meta-analysis, Journal of Clinical Epidemiology, 2024, Autier P et al. PubMed [Evidence: A]
- 3 . Meta-analysis of breast cancer mortality benefit and overdiagnosis adjusted for adherence, British Journal of Cancer, 2016, Jacklyn G et al. PubMed [Evidence: A]
- 4 . Annual mammographic screening to reduce breast cancer mortality: UK Age RCT, Health Technology Assessment, 2020, Duffy SW et al. PubMed [Evidence: B]
- 5 . Impact of digital breast tomosynthesis on screening performance: A meta-analysis, PLoS One, 2025, Liu X et al. PubMed [Evidence: A]
- 6 . Accuracy of Digital Breast Tomosynthesis (TOMMY Trial), Radiology, 2015, Gilbert FJ et al. PubMed [Evidence: C]
- 7 . Comparing accuracy of tomosynthesis (MAITA RCT consortium), European Journal of Cancer, 2024, Rossi PG et al. PubMed [Evidence: B]
- 8 . Oslo Tomosynthesis Screening Trial interpretations, European Radiology, 2024, Skaane P et al. PubMed [Evidence: C]
- 9 . Factors Associated With False-Positive and False-Negative Results, Annals of Internal Medicine, 2016, Nelson HD et al. PubMed [Evidence: C]
- 10 . Screening mammographic performance by race and age, Breast Cancer Research and Treatment, 2024, Lee CS et al. PubMed [Evidence: C]
- 11 . Screening mammography performance: radiologists versus AI, Breast Cancer Research, 2024, Kwon MR et al. PubMed [Evidence: C]
- 12 . Sensitivity of screening mammography by density and texture, Breast Cancer Research, 2019, von Euler-Chelpin M et al. PubMed [Evidence: C]
- 13 . The epidemiology, radiology and biological characteristics of interval breast cancers, NPJ Breast Cancer, 2017, Houssami N et al. PubMed [Evidence: C]
- 14 . Breast Cancer Induced by X-Ray Mammography Screening?, Medical Principles and Practice, 2016, Pauwels EKJ et al. PubMed [Evidence: C]
- 15 . Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement, JAMA, 2024, Nicholson WK et al. PubMed [Evidence: D]
- 16 . Screening for Breast Cancer: Evidence Report for the US Preventive Services Task Force, JAMA, 2024, Henderson JT et al. PubMed [Evidence: D]
Medical Disclaimer
This content is for informational and educational purposes only. It is not intended to provide medical advice or to take the place of such advice or treatment from a personal physician. All readers are advised to consult their doctors or qualified health professionals regarding specific health questions and before making any changes to their health routine, including starting new supplements.
Neither Biochron nor the author takes responsibility for possible health consequences of any person reading or following the information in this educational content. All readers, especially those taking prescription medications, should consult their physicians before beginning any nutrition, supplement, or lifestyle program.
If you have a medical emergency, call your doctor or emergency services immediately.
