

💡 What You Need to Know Right Away
Carotid Doppler is an ultrasound test that uses sound waves to measure blood flow through the carotid arteries in your neck, helping doctors detect blockages and plaque buildup that could increase your risk of stroke.
Also known as: Carotid Ultrasound, Carotid Duplex, Carotid Duplex Scan, Carotid Artery Ultrasound
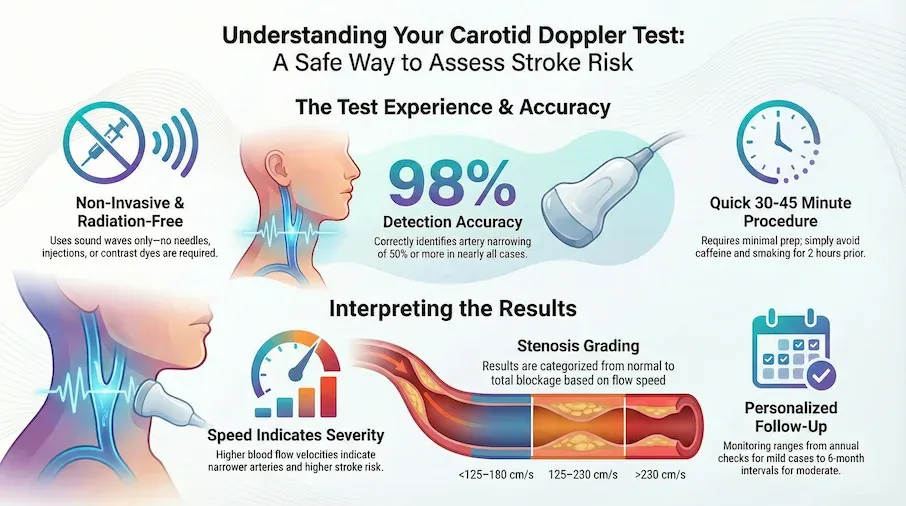
- Research shows this test correctly identifies artery narrowing of 50% or more in about 98 out of 100 cases[Evidence: A][1]
- The test detects complete artery blockages with 95% accuracy[Evidence: A][3]
- Blood flow speeds above 230 cm/s indicate severe narrowing (70% or more) with 99% sensitivity[Evidence: A][2]
- The procedure is painless, radiation-free, and takes 30 to 45 minutes to complete
If your doctor has recommended a carotid Doppler test, you may be wondering what the procedure involves and what your results will mean. It is common to feel anxious about medical tests, especially ones related to stroke risk.
The good news is that carotid Doppler is one of the safest and most informative tests available for evaluating your artery health. Unlike CT scans or MRIs, this ultrasound test uses no radiation and requires no injections or contrast dye. Most people find the experience similar to a routine prenatal ultrasound.
In this guide, you will learn exactly what happens during the test, how to interpret your results, and what the different stenosis categories mean for your health. Whether you are preparing for your first carotid Doppler or trying to understand results you have already received, this article provides the evidence-based information you need.
❓ Quick Answers
What is a carotid Doppler test?
Carotid Doppler is a painless ultrasound test that measures blood flow through the carotid arteries in your neck. The test helps doctors detect narrowing (stenosis), plaque buildup, and blockages that could increase your risk of stroke. It combines B-mode imaging (which shows artery structure) with Doppler analysis (which measures blood flow speed).
Is carotid Doppler safe?
Carotid Doppler is extremely safe. The test uses sound waves only, with no radiation, needles, or contrast dye. There are no known risks or side effects from standard carotid ultrasound. In nearly 50 years of clinical use, carotid ultrasound has proven risk-free for virtually all patients.
How accurate is carotid Doppler?
Research shows carotid Doppler correctly identifies artery narrowing of 50% or more in about 98 out of 100 cases[Evidence: A][1]. For severe narrowing (70% or more), updated blood flow speed thresholds achieve 90 to 99% sensitivity[Evidence: B][11]. The test also detects complete blockages with 95% accuracy[Evidence: A][3].
How long does a carotid Doppler take?
A complete bilateral carotid Doppler study typically takes 30 to 45 minutes. This includes time for positioning, gel application, and scanning both sides of your neck. You will receive your results either immediately after the test or within a few days, depending on your facility.
What does a carotid Doppler show?
Carotid Doppler reveals the structure and blood flow in your carotid arteries. It detects plaque buildup (fatty deposits on artery walls), stenosis (narrowing of the artery), blood flow velocity, and artery wall thickness. These findings help doctors assess your stroke risk and determine treatment options.
Do I need to prepare for a carotid Doppler?
Preparation is minimal. There are no food or drink restrictions. Continue taking your regular medications unless told otherwise. Avoid caffeine and smoking for 2 hours before the test. Wear a loose, open-neck shirt and remove necklaces before arrival.
What is a normal carotid Doppler result?
Normal results show blood flow speeds (peak systolic velocity) below 125 to 180 cm/s, depending on your lab's criteria[Evidence: B][9]. Normal findings indicate no significant narrowing, with smooth artery walls and no flow disturbances. Your doctor will explain what your specific numbers mean for your situation.
What happens if my carotid Doppler is abnormal?
Abnormal results are categorized by severity. Mild narrowing (less than 50%) typically requires lifestyle changes and annual monitoring[Evidence: D][7]. Moderate narrowing (50 to 69%) may need medication and monitoring every 6 months. Severe narrowing (70% or more) often requires evaluation for surgery or stenting. Your doctor will discuss next steps based on your specific findings.
Carotid Doppler Test
A non-invasive ultrasound procedure used to examine the blood flow in the carotid arteries, helping to identify blockages and stroke risks.
🔬 How Does Carotid Doppler Work?
Carotid Doppler combines two ultrasound technologies to create a complete picture of your artery health. Understanding how the test works can help you feel more comfortable during the procedure.
B-Mode Imaging: Seeing the Artery Structure
Think of B-mode ultrasound like a flashlight shining into a dark tunnel. The sound waves bounce off the artery walls and return to the transducer, creating a grayscale image of your artery's interior. This allows the sonographer to see plaque deposits, measure artery wall thickness, and identify structural abnormalities.
Doppler Flow Analysis: Measuring Blood Speed
The Doppler component works like a speed detector for your blood. When sound waves hit moving red blood cells, they bounce back at a different frequency. This frequency shift reveals exactly how fast blood is flowing through your arteries. Research shows that blood flow speeds correlate directly with the degree of artery narrowing[Evidence: B][11].
Color Doppler Imaging
Color Doppler adds visual information by displaying blood flow direction and speed as colors on the screen. Typically, blood flowing toward the transducer appears red, while blood flowing away appears blue. Turbulent flow (which suggests narrowing) shows as a mosaic of colors. This helps the sonographer quickly identify problem areas.
Why Blood Flow Speed Matters
Imagine water flowing through a garden hose. If you pinch the hose, water speeds up at the narrowed point. The same principle applies to your arteries. When plaque narrows a carotid artery, blood must flow faster to maintain the same volume. Established velocity criteria grade stenosis severity based on peak systolic velocity (PSV) measurements[Evidence: A][2]. A comprehensive review of 22 studies with nearly 5,000 carotid arteries confirmed the reliability of these measurements[Evidence: A][3].
Plaque Characterization
Modern carotid Doppler also analyzes plaque composition. Research shows that plaque characteristics significantly predict stroke risk[Evidence: A][10]. Studies indicate that people with bleeding inside their artery plaque had about 3 times higher stroke risk compared to those with calcified plaque[Evidence: A][10]. Standardized measurement criteria improve consistency between different testing centers[Evidence: C][8].
🧪 What to Expect: The Real User Experience
During the Procedure
You will lie on an examination table with your head positioned on a pillow, turned about 45 degrees to one side. The room may feel cool, which is common in radiology departments. The sonographer applies warm ultrasound gel to your neck, typically at body temperature (98 to 100°F) or slightly warmer.
The transducer applies light to moderate pressure on your neck, similar to a firm handshake. Some patients describe it as "someone gently pressing their thumb against your neck." The sonographer moves the transducer along both sides of your neck, adjusting pressure over deeper artery segments. The test is not painful, though you may notice mild discomfort if you are sensitive to neck touch or have difficulty lying still.
You will hear distinctive rhythmic "swish-swish" or "whoosh-whoosh" sounds when the Doppler component activates. This sound represents blood flow through your arteries. The pitch changes with blood velocity, and sounds may be louder over areas of turbulent flow. Some people find this sound reassuring, as they can hear their blood flowing. The sonographer can adjust the volume if needed.
What You Will Feel After
- Mild neck stiffness from the 45-degree head positioning, which typically resolves within 15 to 30 minutes with gentle stretching
- Slight gel residue near your ears if not thoroughly cleaned, which washes off with soap and water
- No bruising, soreness, or skin reactions since the test is completely non-invasive
- No activity restrictions. You can drive home and return to normal activities immediately
How to Make It Easier
- For neck strain: Request an extra pillow under your neck if the position feels uncomfortable
- If the room is cold: Ask the technologist for a blanket, which is standard practice in most facilities
- For anxiety: Practice slow, deep breathing throughout the procedure. No breath-holding is required
- For sound sensitivity: Bring headphones or music (ask about facility policy first)
- Before arriving: Wear a loose, open-neck shirt to avoid changing into a gown
- To prepare: Remove necklaces and earrings before the test to avoid interference with transducer movement
📊 Preparation and Procedure
Before Your Test
| Preparation Item | Recommendation |
|---|---|
| Food and drink | No restrictions. Eat and drink normally |
| Medications | Continue all medications unless told otherwise by your doctor |
| Caffeine | Avoid for 2 hours before the test |
| Smoking | Stop smoking for 2 hours before the test |
| Clothing | Wear a loose, open-neck shirt or blouse |
| Jewelry | Remove necklaces before the test |
| Skin preparation | Arrive with clean neck area. Avoid lotions, powders, or perfumes |
Stenosis Grading Criteria
Your results are interpreted using standardized velocity thresholds. Studies indicate established blood flow speed measurements accurately grade artery narrowing according to stroke prevention trial standards[Evidence: A][2].
| Stenosis Category | Peak Systolic Velocity | Plain Language | Evidence |
|---|---|---|---|
| Normal or minimal (<50%) | <125-180 cm/s | Little to no significant narrowing | [B][9] |
| Moderate (50-69%) | 125-230 cm/s | Moderate narrowing that may need medication | [A][1] |
| Severe (≥70%) | >230 cm/s | Severe narrowing requiring intervention evaluation | [A][2] |
| Near-occlusion | Variable (may be low) | Almost complete blockage with reduced flow | [B][11] |
| Total occlusion | No flow detected | Complete blockage, no blood flow | [A][3] |
Important note: Studies suggest using a blood flow speed of 180 cm/s or higher improves the test's ability to detect narrowing of at least 50%[Evidence: B][9]. With this updated threshold, the test correctly identified narrowing in about 93 out of 100 cases[Evidence: B][9]. Your facility may use slightly different thresholds based on their internal validation.
⚠️ Safety Information
Carotid Doppler is one of the safest diagnostic tests available. The procedure uses sound waves only, with no radiation exposure. There are no known risks or serious side effects from standard carotid ultrasound.
When This Test Is Most Helpful
Clinical guidelines emphasize this test is most helpful for people with symptoms like mini-strokes or those at high risk for stroke[Evidence: D][6]. Expert consensus indicates screening may cause more harm than benefit in people at low risk for stroke[Evidence: D][6].
Understanding Your Risk
Research shows that plaque characteristics help predict future events. Studies suggest bleeding inside artery plaque is an independent risk factor for another stroke or mini-stroke[Evidence: B][12]. Additionally, larger total plaque volume predicts the chance of another stroke or mini-stroke happening[Evidence: B][12].
When to Seek Immediate Care
Contact emergency services immediately if you experience:
- Sudden symptoms: Sudden weakness on one side, vision loss, severe headache, slurred speech, or difficulty understanding speech
- TIA symptoms: Brief episodes of the above that resolve within minutes (these are medical emergencies)
Contact your doctor soon if you notice:
- Worsening dizziness or balance problems
- Frequent brief episodes of visual disturbance
- Progressive symptoms that were previously stable
🥗 Practical Guidance for Your Results
Surveillance Schedule Based on Results
Clinical guidelines provide clear recommendations for follow-up based on your stenosis severity:
- Mild narrowing (<50%): Clinical guidelines recommend annual ultrasound monitoring[Evidence: D][7]. Focus on lifestyle changes including diet, exercise, and smoking cessation
- Moderate narrowing (50-79%): Clinical guidelines recommend ultrasound checks every 6 months[Evidence: D][7]. Your doctor may prescribe cholesterol-lowering medication and antiplatelet therapy
- Severe narrowing (≥70%): Requires evaluation for surgical intervention (carotid endarterectomy) or stenting. Follow-up schedule determined by your vascular surgeon
- After carotid surgery: Standard practice includes a baseline ultrasound within 30 days after carotid artery surgery to monitor healing[Evidence: D][7]
Making Sense of Plaque Findings
Research shows this test is useful for finding early signs of artery disease before symptoms appear[Evidence: A][4]. Studies indicate analyzing plaque characteristics with this test helps doctors better predict heart and stroke risk[Evidence: A][4]. Research shows plaque height of 1.5 millimeters or more on ultrasound was associated with increased risk of heart and stroke events[Evidence: A][4].
Questions to Ask Your Doctor
- What is my stenosis percentage, and which category does it fall into?
- Did the test show any concerning plaque characteristics?
- Based on my results, what lifestyle changes should I prioritize?
- Do I need medication, and if so, what are the options?
- When should I schedule my next carotid Doppler?
- Should I see a vascular specialist based on these findings?
What to Look for When Choosing a Carotid Doppler Provider
The quality of your test results depends on the lab and healthcare provider. Here is what to consider:
Lab Quality Markers
- IAC or ICAVL accreditation: Intersocietal Accreditation Commission (IAC) or ICAVL certification for vascular testing Why it matters: Accredited labs meet rigorous quality standards for equipment, staff training, and testing protocols
- Standardized velocity criteria: Lab should use validated consensus panel criteria[Evidence: C][8] Why it matters: Standardization improves inter-laboratory consistency and result reliability
- Registered vascular technologists (RVT): Sonographers should hold RVT credential from ARDMS Why it matters: Certified technologists have demonstrated competency in vascular ultrasound
- Physician interpretation: Results should be interpreted by a physician trained in vascular ultrasound Why it matters: Proper interpretation requires specialized expertise in vascular disease
Questions to Ask Your Provider
- Is your vascular lab accredited by IAC or ICAVL?
- What velocity criteria does your lab use (SRU consensus, IAC updated thresholds)?
- Are your sonographers registered vascular technologists?
- When will I receive my results, and who will explain them?
- What is the cost if my insurance does not cover it?
Red Flags to Avoid
- No accreditation: Unaccredited labs may lack quality oversight and standardized protocols
- Unusually quick exams: A complete bilateral study should take 30 to 45 minutes. Significantly shorter exams may be incomplete
- No physician interpretation: Results should include formal interpretation by a qualified physician
- Pressure for additional testing: Be cautious of facilities that routinely recommend expensive follow-up tests without clear medical indication
How Carotid Doppler Compares to Other Tests
Carotid Doppler, CT angiography (CTA), and MR angiography (MRA) all evaluate carotid arteries, but they have different strengths. Carotid Doppler is the first-line test because it is non-invasive, cost-effective, and widely available.
| Feature | Carotid Doppler | CT Angiography | MR Angiography |
|---|---|---|---|
| Invasiveness | Non-invasive (no needles, no contrast) | Minimally invasive (IV contrast required) | Non-invasive or minimally invasive (contrast optional) |
| Radiation | None (uses sound waves) | Yes (X-ray radiation) | None (uses magnetic fields) |
| Agreement with gold standard | 79% concordance with CTA[Evidence: B][5] | Reference standard for stenosis grading | 92% sensitivity vs CTA[Evidence: B][5] |
| Limitations | May underestimate stenosis in 14% of cases[Evidence: B][5] | Requires IV contrast (kidney concerns), radiation exposure | Cannot be performed with certain implants, claustrophobia issues |
| Cost (relative) | $ (lowest cost) | $$ to $$$ (moderate) | $$$ (highest cost) |
| Best for | Initial screening, surveillance, patients avoiding radiation | Surgical planning, confirming severe stenosis | Patients with contrast allergies, need for detailed soft tissue |
Studies suggest carotid Doppler remains a cost-effective first choice for evaluating carotid arteries[Evidence: B][5]. When results are borderline or surgical intervention is planned, your doctor may order CT or MR angiography to confirm findings.
What The Evidence Shows (And Does Not Show)
What Research Suggests
- Carotid Doppler correctly identifies moderate stenosis (≥50%) with 93 to 98% sensitivity depending on velocity thresholds used[Evidence: A][1][9]
- For severe stenosis (≥70%), using PSV thresholds of 200 to 230 cm/s achieves 90 to 99% sensitivity and 86 to 94% specificity[Evidence: A][2][11]
- Complete arterial occlusion is detected with 95% sensitivity and 91% specificity (based on 22 studies with nearly 5,000 carotid arteries)[Evidence: A][3]
- Plaque characterization significantly improves cardiovascular risk prediction beyond stenosis degree alone[Evidence: A][4][10]
- Intraplaque hemorrhage increases stroke risk approximately 3-fold compared to calcified plaques[Evidence: A][10]
What Is NOT Yet Proven
- Optimal velocity thresholds vary by laboratory. The IAC 2021 criteria (≥180 cm/s for 50% stenosis) differ from earlier SRU consensus criteria (≥125 cm/s)
- Long-term stroke prevention benefit of screening asymptomatic low-risk populations has not been established in randomized trials
- Inter-laboratory variability remains a limitation. Results from different facilities may not be directly comparable without local validation
- The role of advanced plaque characterization in routine clinical decision-making is still evolving
Where Caution Is Needed
- Carotid Doppler may underestimate stenosis in about 14% of cases and overestimate in about 7%[Evidence: B][5]
- Concordance with CT angiography is approximately 79%, meaning discrepancies occur in about 1 in 5 cases[Evidence: B][5]
- Clinical guidelines recommend against routine screening in asymptomatic adults without risk factors[Evidence: D][6]
Should YOU Get This Test?
Best suited for: People who have experienced stroke symptoms, TIA, or have a carotid bruit detected on physical exam. Also appropriate for monitoring known carotid artery disease and post-surgical surveillance.
Not recommended for: General population screening without symptoms or high-risk factors. Guidelines recommend against routine carotid screening in asymptomatic low-risk individuals.
Realistic timeline: Results are typically available immediately or within a few days. Follow-up depends on findings (annual for mild stenosis, 6-month intervals for moderate stenosis).
When to consult a professional: Consult your doctor if you have experienced stroke-like symptoms (even if brief), have high blood pressure, diabetes, or high cholesterol, smoke, or have a family history of stroke or carotid artery disease.
Frequently Asked Questions
Can I eat or drink before a carotid Doppler?
Yes, there are no food or drink restrictions before a carotid Doppler test. You can eat and drink normally on the day of your appointment. The only recommendations are to avoid caffeine and smoking for about 2 hours before the test, as these can temporarily affect blood flow measurements. Continue taking all your regular medications unless your doctor specifically tells you otherwise.
Does Medicare cover carotid Doppler tests?
Medicare Part B typically covers carotid Doppler ultrasound when medically necessary, such as after a stroke, TIA, or when your doctor detects a carotid bruit (abnormal sound). Coverage usually applies at 80% of the Medicare-approved amount after you meet your annual deductible. Screening in asymptomatic individuals without risk factors may not be covered, as clinical guidelines recommend against routine screening in the general population. Check with your Medicare plan for specific coverage details.
How often should I get a carotid Doppler test?
The frequency depends on your results and risk factors. For mild narrowing (less than 50%), clinical guidelines recommend annual ultrasound monitoring. For moderate narrowing (50 to 79%), guidelines recommend checks every 6 months. After carotid surgery, a baseline ultrasound is recommended within 30 days, with ongoing surveillance based on your surgeon's recommendations. If you have no known carotid disease, screening is generally not recommended without symptoms or high-risk factors.
What is the difference between carotid Doppler and transcranial Doppler?
Carotid Doppler examines the carotid arteries in your neck (extracranial arteries), while transcranial Doppler (TCD) examines arteries inside your skull (intracranial arteries). The probe placement differs: carotid Doppler uses probes on the sides of your neck, while TCD uses probes on your temples, behind your ears, or sometimes through your eyelids. Carotid Doppler primarily detects stenosis and plaque, while TCD is often used to detect microemboli, monitor for vasospasm after bleeding, and assess blood flow in stroke patients. Your doctor may order one or both tests depending on your clinical situation.
Can carotid Doppler detect stroke risk?
Yes, carotid Doppler is one of the primary tools for assessing stroke risk. The test identifies carotid artery narrowing, which is a major risk factor for ischemic stroke. Research shows that plaque characteristics also predict stroke risk. Studies indicate that people with bleeding inside their artery plaque had about 3 times higher stroke risk compared to those with calcified plaque. Additionally, detailed plaque characteristics help doctors make better treatment decisions even when narrowing is mild to moderate.
What if my carotid Doppler results differ from a previous test?
Some variation between tests is normal due to differences in equipment, sonographer technique, and physiological factors like blood pressure at the time of testing. If your results change significantly, your doctor may recommend additional imaging (CT or MR angiography) to clarify findings. Standardized measurement criteria improve consistency between different testing centers, but some inter-laboratory variation still occurs. Discuss any concerns with your doctor, who can interpret results in the context of your overall clinical picture.
Is carotid Doppler accurate for severe stenosis?
Yes, carotid Doppler is highly accurate for detecting severe stenosis. Research shows when blood flow speeds exceeded 230 cm/s, this test identified severe narrowing (70% or more) in 99 out of 100 cases. A more recent validation study found that using a blood flow speed of 200 cm/s as the cut-off for severe narrowing correctly identified it in about 90 out of 100 cases with 94% specificity. For surgical planning, doctors may still order CT or MR angiography to confirm findings.
What should I do if I have mild stenosis found on carotid Doppler?
Mild stenosis (less than 50% narrowing) is typically managed with lifestyle modifications and risk factor control. Focus on a heart-healthy diet, regular exercise, smoking cessation, and blood pressure management. Your doctor may prescribe cholesterol-lowering medication (statins) and low-dose aspirin depending on your overall cardiovascular risk. Annual surveillance with carotid Doppler is recommended to monitor for progression. Surgery is generally not recommended for mild stenosis because the risks outweigh the benefits at this stage.
Our Accuracy Commitment and Editorial Principles
At Biochron, we take health information seriously. Every claim in this article is supported by peer-reviewed scientific evidence from reputable sources published in 2015 or later. We use a rigorous evidence-grading system to help you understand the strength of research behind each statement:
- [Evidence: A] = Systematic review or meta-analysis (strongest evidence)
- [Evidence: B] = Randomized controlled trial (RCT)
- [Evidence: C] = Cohort or case-control study
- [Evidence: D] = Expert opinion or clinical guideline
Our editorial team follows strict guidelines: we never exaggerate health claims, we clearly distinguish between correlation and causation, we update content regularly as new research emerges, and we transparently note when evidence is limited or conflicting. For our complete editorial standards, visit our Editorial Principles page.
This article is for informational purposes only and does not constitute medical advice. Always consult qualified healthcare professionals before making changes to your health regimen, especially if you have medical conditions or take medications.





References
- 1 . Sensitivity and specificity of color duplex ultrasound measurement in the estimation of internal carotid artery stenosis: a systematic review and meta-analysis, Journal of vascular surgery, 2005, Jahromi AS, Cinà CS, Liu Y, Clase CM. PubMed [Evidence: A]
- 2 . Accuracy of the Society of Radiologists in Ultrasound (SRU) Carotid Doppler Velocity Criteria for Grading North American Symptomatic Carotid Endarterectomy Trial (NASCET) Stenosis: A Meta-Analysis, Journal of ultrasound in medicine, 2023, Polak JF, Alexandrov AV. PubMed [Evidence: A]
- 3 . Duplex ultrasound for diagnosing symptomatic carotid stenosis in the extracranial segments, The Cochrane database of systematic reviews, 2022, Cassola N, Baptista-Silva JC, Nakano LC, et al. PubMed [Evidence: A]
- 4 . Usefulness of Carotid Ultrasound Screening in Primary Cardiovascular Prevention: A Systematic Review, Current problems in cardiology, 2024, Sebastian SA, Co EL, Tidd-Johnson A, et al. PubMed [Evidence: A]
- 5 . Imaging of Carotid Stenosis: Where Are We Standing? Comparison of Multiparametric Ultrasound, CT Angiography, and MRI Angiography, with Recent Developments, Diagnostics (Basel, Switzerland), 2024, David E, Grazhdani H, Aliotta L, et al. PubMed [Evidence: B]
- 6 . Screening for Asymptomatic Carotid Artery Stenosis: US Preventive Services Task Force Recommendation Statement, JAMA, 2021, US Preventive Services Task Force. PubMed [Evidence: D]
- 7 . Society for Vascular Surgery clinical practice guidelines for management of extracranial cerebrovascular disease, Journal of vascular surgery, 2022, AbuRahma AF, Avgerinos ED, Chang RW, et al. PubMed [Evidence: D]
- 8 . Carotid Consensus Panel duplex criteria can replace modified University of Washington criteria without affecting accuracy, Vascular medicine, 2018, Kim AH, Augustin G, Shevitz A, et al. PubMed [Evidence: C]
- 9 . Optimization of duplex velocity criteria for diagnosis of internal carotid artery (ICA) stenosis: A report of the Intersocietal Accreditation Commission (IAC) Vascular Testing Division Carotid Diagnostic Criteria Committee, Vascular medicine, 2021, Gornik HL, Rundek T, Gardener H, et al. PubMed [Evidence: B]
- 10 . Carotid plaque components and other carotid artery features associated with risk of stroke: A systematic review and meta-analysis, Journal of stroke and cerebrovascular diseases, 2022, Zhang Y, Bai Y, Xie J, et al. PubMed [Evidence: A]
- 11 . Correlation between Ultrasound Peak Systolic Velocity and Angiography for Grading Internal Carotid Artery Stenosis, Journal of clinical medicine, 2024, Tătaru DA, Olinic M, Homorodean C, et al. PubMed [Evidence: B]
- 12 . Carotid Plaque Characteristics Predict Recurrent Ischemic Stroke and TIA: The PARISK (Plaque At RISK) Study, JACC. Cardiovascular imaging, 2022, van Dam-Nolen DHK, Truijman MTB, van der Kolk AG, et al. PubMed [Evidence: B]
Medical Disclaimer
This content is for informational and educational purposes only. It is not intended to provide medical advice or to take the place of such advice or treatment from a personal physician. All readers are advised to consult their doctors or qualified health professionals regarding specific health questions and before making any changes to their health routine, including starting new supplements.
Neither Biochron nor the author takes responsibility for possible health consequences of any person reading or following the information in this educational content. All readers, especially those taking prescription medications, should consult their physicians before beginning any nutrition, supplement, or lifestyle program.
If you have a medical emergency, call your doctor or emergency services immediately.
