

💡 What You Need to Know Right Away
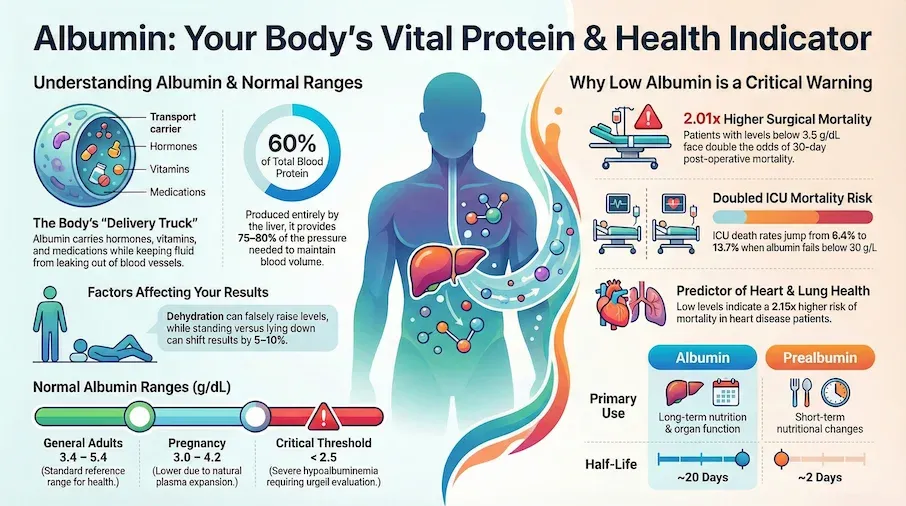
- Low albumin doubles mortality risk in surgical patients. Patients with albumin below 3.5 g/dL had 2.01 times higher odds of 30-day mortality in a study of over 842,000 patients.[Evidence: C][3]
- Critical care patients with low albumin face significantly worse outcomes. ICU mortality was 13.7% for patients with albumin below 30 g/L compared to 6.4% for those with normal levels.[Evidence: C][4]
- Albumin testing helps predict heart disease outcomes. Patients with acute coronary syndrome and low albumin had 2.15 times higher risk of all-cause mortality.[Evidence: A][5]
- Albumin-based indices show strong prognostic value. Multiple albumin ratios predict mortality in heart failure patients better than albumin alone.[Evidence: A][8]
An albumin blood test is a diagnostic laboratory test that measures the amount of albumin protein in your blood. Albumin is produced by your liver and maintains fluid balance in blood vessels while transporting vitamins, hormones, and enzymes throughout your body. The test is typically used to assess liver function, kidney function, and nutritional status through a simple blood draw.
If your doctor has ordered an albumin test, you may be wondering what your results mean for your health. It is common to feel anxious while waiting for lab results, especially when you do not fully understand what is being measured. This comprehensive guide will help you understand why albumin testing matters, what normal and abnormal results indicate, and when you should seek medical attention. You will learn how this simple blood test can provide crucial insights into your liver health, kidney function, and overall nutritional status.
❓ Quick Answers
What is albumin in a blood test?
Albumin is a protein made by your liver that makes up about 60% of your blood's total protein content. A blood albumin test measures this protein level to assess liver function, kidney health, and nutritional status. Normal adult levels range from 3.4 to 5.4 g/dL. The test requires a simple blood draw and results are typically available within 12-24 hours.
What is a normal albumin level?
Normal albumin levels for adults range from 3.4 to 5.4 g/dL (34-54 g/L). For elderly patients, normal ranges are slightly lower at 3.4 to 4.8 g/dL. During pregnancy, normal levels decrease to 3.0 to 4.2 g/dL. Levels below 3.5 g/dL are considered low and may indicate health concerns requiring medical evaluation.[Evidence: C][3]
Do I need to fast for an albumin test?
No, fasting is not required for a standalone albumin blood test. However, if albumin is being measured as part of a comprehensive metabolic panel (CMP), your doctor may request 8-12 hours of fasting. Always follow your healthcare provider's specific preparation instructions. Staying well-hydrated before the test helps make blood collection easier.
How long does an albumin test take?
The blood draw itself takes only 2-5 minutes. A healthcare professional will insert a needle into a vein, usually in your arm, and collect a small blood sample. Results are typically available within 12-24 hours, depending on the laboratory. If ordered urgently in a hospital setting, results may be available within a few hours.
What does low albumin indicate?
Low albumin (hypoalbuminemia) may indicate liver disease, kidney disease, malnutrition, inflammation, or infection. In critically ill patients, albumin below 30 g/L was associated with significantly higher ICU mortality (13.7% vs 6.4%).[Evidence: C][4] Severe hypoalbuminemia below 2.5 g/dL requires prompt medical evaluation.
What does high albumin mean?
High albumin (hyperalbuminemia) is less common than low albumin and usually indicates dehydration rather than overproduction. When your body loses fluid through vomiting, diarrhea, or inadequate water intake, albumin becomes more concentrated in your blood. Rarely, high albumin may occur with high-protein diets. Treatment typically involves rehydration.
Is albumin part of a comprehensive metabolic panel?
Yes, albumin is included in the comprehensive metabolic panel (CMP), which measures 14 different substances in your blood. The CMP also includes glucose, electrolytes, kidney function markers, and liver enzymes. Albumin can also be ordered as a standalone test or as part of a liver function panel when specific liver assessment is needed.
Albumin Blood Test
Albumin is the most abundant protein in blood plasma, produced entirely by the liver. This essential test is crucial for evaluating your overall health, nutritional status, and vital organ function.
🔬 How Albumin Works in Your Body
Think of albumin as the delivery truck of your bloodstream. Just as trucks transport goods across highways, albumin carries essential substances like hormones, vitamins, calcium, and medications throughout your body. Without enough delivery trucks, goods pile up in some areas while other areas go without, and this is similar to what happens when albumin levels drop too low.
Your liver produces approximately 10-15 grams of albumin daily. This protein serves three critical functions in your body. First, albumin maintains oncotic pressure, the force that keeps fluid inside your blood vessels rather than leaking into surrounding tissues. When albumin drops, fluid escapes into tissues, causing swelling (edema) in the legs, ankles, and abdomen.
Second, albumin acts as a transport protein. It binds to and carries substances that cannot dissolve easily in blood, including fatty acids, bilirubin, and many medications. This binding affects how drugs work in your body, which is why doctors monitor albumin in patients taking certain medications.
Third, albumin provides approximately 75-80% of the oncotic pressure needed to maintain proper blood volume. Research demonstrates that each 10 g/L decrease in albumin is associated with a 137% increase in mortality odds in critically ill patients.[Evidence: C][4] This makes albumin one of the most important prognostic markers in hospital settings.
A meta-analysis of over 21,000 patients with acute coronary syndrome found that low albumin independently predicted all-cause mortality with a risk ratio of 2.15 (95% CI: 1.68-2.75).[Evidence: A][5] Similarly, in COVID-19 patients, hypoalbuminemia showed an odds ratio of 6.97 for composite poor outcomes with a diagnostic sensitivity of 0.63 and specificity of 0.81.[Evidence: A][12]
📊 Normal Albumin Levels: Reference Ranges
Understanding your albumin test results requires knowing the appropriate reference range for your age and health status. Laboratories may report slightly different ranges based on their testing methods, so always compare your results to the reference range provided on your lab report.
| Population | Normal Range | Clinical Significance | Evidence |
|---|---|---|---|
| Adults (general) | 3.4-5.4 g/dL (34-54 g/L) | Standard reference range | Clinical standard |
| Elderly (≥65 years) | 3.4-4.8 g/dL | Below 2.8 g/dL: highest mortality risk | [A][10] |
| Pregnancy | 3.0-4.2 g/dL | Physiologic decrease due to plasma expansion | Clinical standard |
| Surgical patients | ≥3.5 g/dL (target) | Below 3.4 g/dL: 2x higher 30-day mortality | [C][3] |
| ICU patients | ≥30 g/L (target) | Below 30 g/L: 13.7% vs 6.4% mortality | [C][4] |
| Critical threshold | <2.5 g/dL | Severe hypoalbuminemia, urgent evaluation | Clinical guideline |
In a large study of 842,672 surgical patients, researchers found that an albumin level of 3.4 g/dL optimally distinguished between high-risk and low-risk patients. Those with albumin below 3.5 g/dL had twice the odds of dying within 30 days of surgery (OR 2.01).[Evidence: C][3]
For elderly patients, the prognostic significance of albumin becomes even more pronounced. A meta-analysis found that albumin below 2.8 g/dL was associated with the highest mortality risk in older adults, with anemia and hypoalbuminemia having additive negative effects on survival.[Evidence: A][10]
⚠️ Risks, Warning Signs, and When to Seek Care
Test-Related Risks
The albumin blood test carries minimal risks. You may experience slight pain or bruising at the needle insertion site. Rarely, some people feel lightheaded during blood draws. Serious complications are extremely uncommon.
Situations That May Affect Results
- Dehydration: Can falsely elevate albumin levels
- IV fluid administration: May dilute blood and lower measured albumin
- Posture: Standing versus lying down can affect results by 5-10%
- Recent albumin infusion: Therapeutic albumin administration affects levels for 2-3 weeks
Clinical Outcomes Associated with Abnormal Albumin
Research consistently demonstrates that low albumin predicts worse outcomes across multiple clinical settings:
- Surgical patients: Hypoalbuminemia increased ICU stay by 1.18 days and hospital stay by 3.34 days in cardiac surgery patients.[Evidence: A][11]
- Head and neck cancer surgery: Low albumin independently predicted ICU-level complications (OR 1.64).[Evidence: C][6]
- Lung cancer: Elevated albumin-bilirubin (ALBI) grade was associated with 2.5 times higher risk of death (HR 2.50) and 1.91 times higher risk of disease progression.[Evidence: A][7]
- Stroke: Hypoalbuminemia is a strong independent prognostic marker associated with increased long-term mortality and worse functional outcomes.[Evidence: A][9]
- COVID-19: Patients with low albumin had 6.26 times higher odds of mortality.[Evidence: A][12]
🩺 When to Get an Albumin Blood Test
Common Reasons Doctors Order This Test
- Liver disease evaluation: Albumin is a marker of liver synthetic function
- Kidney disease monitoring: Nephrotic syndrome causes albumin loss in urine
- Nutritional assessment: Malnutrition decreases albumin production
- Pre-surgical risk assessment: Low albumin predicts surgical complications[3]
- Critical illness monitoring: Albumin tracks disease severity in ICU settings[4]
- Cirrhosis management: Guides albumin replacement therapy decisions[1]
Preparation for Your Test
- Fasting: Not required for albumin alone. If part of CMP, follow your doctor's fasting instructions.
- Hydration: Drink normal amounts of water. Dehydration can artificially elevate results.
- Medications: Continue all medications unless your doctor advises otherwise.
- Timing: Albumin levels can vary slightly throughout the day. Consistent timing helps track trends.
What to Expect During the Test
- A healthcare professional cleans the skin over a vein (usually in your arm)
- An elastic band is placed above the site to make veins more visible
- A needle is inserted to collect 5-10 mL of blood (takes 2-5 minutes)
- Pressure is applied to stop bleeding, and a bandage is placed
- Results are typically available within 12-24 hours
Understanding Your Results
When reviewing your albumin results, consider the clinical context. A single measurement provides limited information. Your doctor will interpret results alongside your symptoms, other lab values, and medical history. Trending albumin over time often provides more useful information than a single value.
For patients with cirrhosis, EASL guidelines recommend albumin administration after large-volume paracentesis (removing more than 5 liters of fluid) and for treatment of spontaneous bacterial peritonitis.[Evidence: D][1]
⚖️ Albumin vs. Prealbumin vs. Total Protein
Several blood tests measure proteins, and understanding the differences helps you interpret your results accurately.
| Feature | Albumin | Prealbumin | Total Protein |
|---|---|---|---|
| What it measures | Main blood protein (60% of total) | Thyroid hormone transport protein | All proteins (albumin + globulins) |
| Half-life | ~20 days | ~2 days | Varies by component |
| Best use | Long-term nutritional status, liver/kidney function | Short-term nutritional changes | General protein screening |
| Responds to nutrition | Slowly (weeks) | Rapidly (days) | Variable |
| Normal range (adults) | 3.4-5.4 g/dL | 15-36 mg/dL | 6.0-8.3 g/dL |
| CPT code | 82040 | 84134 | 84155 |
When prealbumin is preferred: Because of its shorter half-life (2 days vs. albumin's 20 days), prealbumin responds faster to nutritional changes. It is often used to monitor nutritional support in hospitalized patients and to assess acute malnutrition.
When albumin is preferred: Albumin better reflects long-term nutritional status and overall liver function. Research shows albumin-based indices, including albumin-globulin ratio and lactate-albumin ratio, provide superior prognostic information in heart failure patients compared to single measurements.[Evidence: A][8]
What The Evidence Shows (And Doesn't Show)
What Research Suggests
- Low albumin is a consistent independent predictor of mortality across multiple clinical settings, including surgery, ICU care, acute coronary syndrome, stroke, heart failure, and COVID-19.[Evidence: A][2][5][9][12]
- Surgical patients with albumin below 3.5 g/dL have approximately twice the odds of 30-day mortality (OR 2.01) based on analysis of 842,672 patients.[Evidence: C][3]
- ICU patients with albumin below 30 g/L experience more than double the mortality rate (13.7% vs. 6.4%) compared to those with higher levels.[Evidence: C][4]
- Albumin treatment in cirrhosis patients with spontaneous bacterial peritonitis reduces mortality by 51% (RR 0.49, n=5,118).[Evidence: A][2]
- For prognostic assessment in COVID-19, hypoalbuminemia demonstrated sensitivity of 0.63, specificity of 0.81, and AUC of 0.77 for poor outcomes.[Evidence: A][12]
What's NOT Yet Proven
- Optimal albumin thresholds for intervention vary by clinical context. The 3.5 g/dL threshold is validated for surgical risk but may differ for other conditions.
- Whether albumin supplementation improves outcomes outside of cirrhosis-specific indications remains under investigation.
- Pediatric-specific albumin reference ranges and prognostic thresholds are not well-established in the evidence reviewed.
- The role of albumin testing in outpatient preventive care versus targeted diagnostic use is not clearly defined.
- Long-term outcomes for patients with borderline low albumin (3.0-3.5 g/dL) are less thoroughly studied than severe hypoalbuminemia.
Where Caution Is Needed
- Albumin is a nonspecific marker. Low levels indicate a problem but do not identify the specific cause without additional testing.
- Acute illness and inflammation can temporarily lower albumin, so isolated low values during illness may not reflect chronic nutritional status.[Evidence: A][12]
- Dehydration and IV fluid administration can falsely alter results. Clinical context is essential for interpretation.
- Using albumin as the sole indicator of nutritional status is insufficient. Prealbumin and clinical assessment provide complementary information.
- Evidence quality varies. Strongest evidence (8 meta-analyses) supports prognostic value. RCTs specifically testing diagnostic protocols are limited.
Should YOU Get This Test?
Best suited for: Patients with suspected liver disease, kidney disease, or malnutrition. Pre-surgical risk assessment. Monitoring critically ill patients. Evaluating unexplained edema or ascites. Part of routine comprehensive metabolic panel.
Not needed for: Routine screening in healthy individuals without specific indications. As a standalone test without clinical context. Frequent repeat testing without clear indication.
Realistic expectations: Results are available within 12-24 hours. A single test provides a snapshot. Trending over time is more informative for chronic conditions. Abnormal results require clinical correlation and usually additional testing.
When to consult a professional: Always discuss results with your healthcare provider. Seek urgent evaluation if albumin is below 2.5 g/dL or accompanied by symptoms like significant swelling, breathing difficulty, or jaundice.
Frequently Asked Questions
What is the difference between albumin and prealbumin?
Albumin and prealbumin are both proteins made by your liver, but they serve different clinical purposes due to their different half-lives. Albumin has a half-life of approximately 20 days, making it useful for assessing long-term nutritional status and chronic liver function. Prealbumin (also called transthyretin) has a half-life of only 2 days, so it responds much faster to nutritional changes. Doctors often order prealbumin when monitoring patients receiving nutritional support in the hospital, while albumin is preferred for routine health assessments and surgical risk stratification.
What is albumin creatinine ratio used for?
The albumin-to-creatinine ratio (ACR) is a urine test, not a blood test, that measures how much albumin is leaking into your urine. Healthy kidneys prevent albumin from passing into urine, so elevated ACR indicates kidney damage. This test is particularly important for people with diabetes or high blood pressure, as these conditions can damage kidney filters. ACR is often ordered alongside blood albumin testing to get a complete picture of both kidney function and overall protein status. The test is recommended annually for people at risk of kidney disease.
How much does an albumin blood test cost?
The cost of a standalone albumin blood test typically ranges from $19 to $52 without insurance, depending on the laboratory and location. When albumin is included in a comprehensive metabolic panel (CMP), the panel typically costs $35 to $100. With insurance, your out-of-pocket cost depends on your plan's deductible and copay structure. Many insurance plans cover albumin testing as part of routine preventive care or when medically necessary. Hospital laboratory costs tend to be higher than independent lab costs. Ask your provider about costs upfront if you are paying out of pocket.
When should I see a doctor for abnormal albumin levels?
Contact your doctor promptly if your albumin level is below 3.0 g/dL or above 5.5 g/dL. Seek urgent medical attention if albumin drops below 2.5 g/dL (severe hypoalbuminemia) or if you develop symptoms such as significant leg swelling, abdominal swelling (ascites), shortness of breath, or yellowing of skin or eyes. Research shows that albumin below 2.8 g/dL carries the highest mortality risk in elderly patients. Your doctor will interpret results in context, as a single mildly abnormal value may simply require repeat testing rather than immediate intervention.
What causes low albumin levels?
Low albumin (hypoalbuminemia) has multiple potential causes. Liver disease reduces albumin production, as the liver manufactures all albumin in the body. Kidney disease, particularly nephrotic syndrome, causes albumin loss in urine. Malnutrition and malabsorption decrease available amino acids for albumin synthesis. Inflammation and infection redirect liver protein production away from albumin. Burns and wounds cause albumin loss through damaged skin. Heart failure may cause fluid overload that dilutes albumin concentration. In critical illness, low albumin is a strong prognostic marker, with hospitalized COVID-19 patients showing 6.26 times higher mortality odds when hypoalbuminemic.
What causes high albumin levels?
High albumin (hyperalbuminemia) is uncommon and almost always indicates dehydration rather than true albumin overproduction. When your body loses fluid through diarrhea, vomiting, excessive sweating, or inadequate water intake, blood becomes more concentrated, artificially raising albumin levels. Rarely, a very high-protein diet may mildly elevate albumin. The treatment for high albumin typically involves rehydration rather than addressing albumin itself. If dehydration is ruled out and albumin remains elevated, your doctor may investigate for rare conditions affecting protein levels.
How is low albumin treated?
Treatment for low albumin depends on the underlying cause. For liver disease such as cirrhosis, EASL guidelines recommend intravenous albumin infusions in specific situations: after large-volume paracentesis (removing more than 5 liters of ascites fluid), for spontaneous bacterial peritonitis, and for hepatorenal syndrome. Meta-analysis shows albumin treatment reduces mortality by 51% in spontaneous bacterial peritonitis. For malnutrition, treatment involves improving protein intake through diet or nutritional supplements. For kidney disease, treating the underlying condition and reducing proteinuria are priorities.
What are symptoms of hypoalbuminemia?
Symptoms of low albumin relate primarily to fluid imbalance. Edema (swelling) in the legs, ankles, and feet occurs because albumin normally keeps fluid inside blood vessels. Ascites (fluid accumulation in the abdomen) develops when severe hypoalbuminemia allows fluid to leak into the abdominal cavity. Fatigue and weakness result from poor nutrition and fluid shifts. Muscle wasting may occur with prolonged protein deficiency. Slow wound healing reflects inadequate protein for tissue repair. Brittle nails and hair loss can indicate chronic protein deficiency. Many people with mild hypoalbuminemia have no symptoms, and the condition is discovered through routine blood testing.
Can dehydration affect albumin levels?
Yes, dehydration significantly affects albumin levels by concentrating the blood. When you lose body water without losing albumin, the measured albumin concentration rises even though total albumin in your body remains unchanged. This is called hemoconcentration. Conversely, overhydration or excessive IV fluids can dilute blood and lower measured albumin levels (hemodilution). For accurate results, maintain normal hydration before your test. If your albumin appears high without other abnormalities, your doctor may recommend repeating the test after ensuring adequate hydration. Posture also affects albumin by 5-10%, with standing positions producing higher readings than lying down.
What medications affect albumin levels?
Several medication categories can influence albumin levels. Anabolic steroids and growth hormone may increase albumin production. Corticosteroids can raise or lower albumin depending on dose and duration. Estrogen-containing medications, including oral contraceptives, may decrease albumin. Nonsteroidal anti-inflammatory drugs (NSAIDs) can cause kidney-related protein loss in some patients. Certain antibiotics affect liver function and thus albumin synthesis. Chemotherapy drugs may reduce albumin through multiple mechanisms. Always inform your doctor about all medications, including supplements, when interpreting albumin results. Albumin also binds many drugs, affecting how medications work in patients with hypoalbuminemia.
Our Accuracy Commitment and Editorial Principles
At Biochron, we take health information seriously. Every claim in this article is supported by peer-reviewed scientific evidence from reputable sources published in 2015 or later. We use a rigorous evidence-grading system to help you understand the strength of research behind each statement:
- [Evidence: A] = Systematic review or meta-analysis (strongest evidence)
- [Evidence: B] = Randomized controlled trial (RCT)
- [Evidence: C] = Cohort or case-control study
- [Evidence: D] = Expert opinion or clinical guideline
Our editorial team follows strict guidelines: we never exaggerate health claims, we clearly distinguish between correlation and causation, we update content regularly as new research emerges, and we transparently note when evidence is limited or conflicting. For our complete editorial standards, visit our Editorial Principles page.
This article is for informational purposes only and does not constitute medical advice. Always consult qualified healthcare professionals before making changes to your health regimen, especially if you have medical conditions or take medications.





References
- 1 . EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. Angeli P, Bernardi M, Villanueva C, et al. Journal of Hepatology, 2018; 69(2):406-460. PubMed | DOI [Evidence: D]
- 2 . Meta-analysis: Efficacy and safety of albumin in the prevention and treatment of complications in patients with cirrhosis. Leache L, Gutiérrez-Valencia M, Saiz LC, et al. Alimentary Pharmacology & Therapeutics, 2023; 57(6):620-634. PubMed | DOI [Evidence: A]
- 3 . The Association between Serum Albumin and Post-Operative Outcomes among Patients Undergoing Common Surgical Procedures. Nipper CA, Lim K, Riveros C, et al. Journal of Clinical Medicine, 2022; 11(21):6543. PubMed | DOI [Evidence: C]
- 4 . Prognostic Value of Serum Albumin Level in Critically Ill Patients: Observational Data From Large Intensive Care Unit Databases. Jin X, Li J, Sun L, et al. Frontiers in Nutrition, 2022; 9:770674. PubMed | DOI [Evidence: C]
- 5 . Serum albumin level for prediction of all-cause mortality in acute coronary syndrome patients: a meta-analysis. Zhu L, Chen M, Lin X. Bioscience Reports, 2020; 40(1):BSR20190881. PubMed | DOI [Evidence: A]
- 6 . Is Preoperative Serum Albumin Predictive of Adverse Outcomes in Head and Neck Cancer Surgery?. Lee CC, Wang TT, Lubek JE, Dyalram D. Journal of Oral and Maxillofacial Surgery, 2023; 81(11):1422-1434. PubMed | DOI [Evidence: C]
- 7 . Prognostic value of albumin-bilirubin grade in lung cancer: a meta-analysis. Jiang J, Li H, Chen L, Qiu X. Journal of Cardiothoracic Surgery, 2024; 19(1):685. PubMed | DOI [Evidence: A]
- 8 . Prognostic value of albumin-based indices for mortality after heart failure: a systematic review and meta-analysis. Jiang J, Miao P, Xin G. BMC Cardiovascular Disorders, 2024; 24(1):570. PubMed | DOI [Evidence: A]
- 9 . Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis. Thuemmler RJ, Pana TA, Carter B, et al. Nutrients, 2024; 16(10):1486. PubMed | DOI [Evidence: A]
- 10 . Serum albumin and health in older people: Review and meta analysis. Cabrerizo S, Cuadras D, Gomez-Busto F, et al. Maturitas, 2015; 81(1):17-27. PubMed | DOI [Evidence: A]
- 11 . Preoperative hypoalbuminemia in patients undergoing cardiac surgery: a meta-analysis. Xu R, Hao M, Zhou W, et al. Surgery Today, 2023; 53(8):861-872. PubMed | DOI [Evidence: A]
- 12 . Prognostic properties of hypoalbuminemia in COVID-19 patients: A systematic review and diagnostic meta-analysis. Soetedjo NNM, Iryaningrum MR, Damara FA, et al. Clinical Nutrition ESPEN, 2021; 45:120-126. PubMed | DOI [Evidence: A]
Medical Disclaimer
This content is for informational and educational purposes only. It is not intended to provide medical advice or to take the place of such advice or treatment from a personal physician. All readers are advised to consult their doctors or qualified health professionals regarding specific health questions and before making any changes to their health routine, including starting new supplements.
Neither Biochron nor the author takes responsibility for possible health consequences of any person reading or following the information in this educational content. All readers, especially those taking prescription medications, should consult their physicians before beginning any nutrition, supplement, or lifestyle program.
If you have a medical emergency, call your doctor or emergency services immediately.
