

💡 What You Need to Know Right Away
3D mammography (tomosynthesis) is a diagnostic imaging test that detects breast cancer earlier, reduces unnecessary callbacks, and provides clearer views of dense breast tissue than standard mammograms.
Also known as: Digital Breast Tomosynthesis (DBT), 3D Mammogram, Breast Tomosynthesis, 3D Breast Imaging
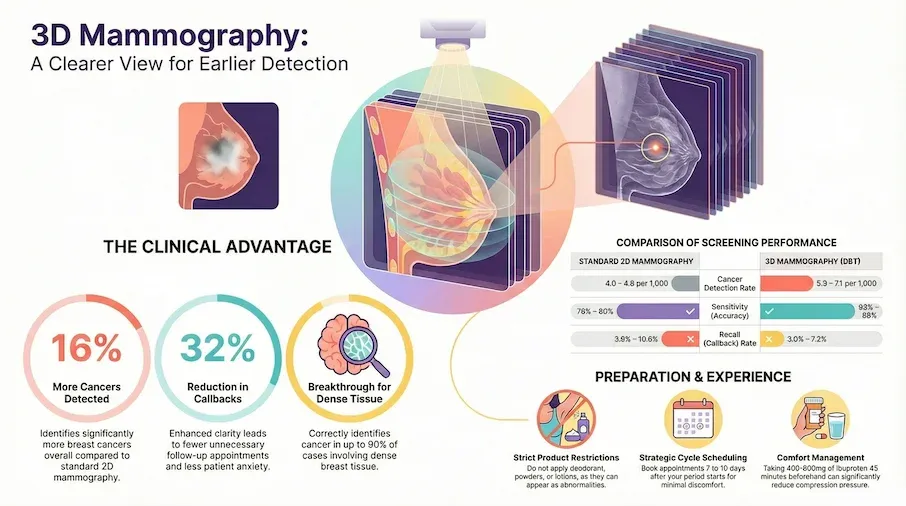
- Research shows 3D mammography detects about 16% more breast cancers overall compared to standard 2D mammography[Evidence: A][1]
- In women with dense breast tissue, 3D mammography correctly identified cancer in about 84 to 90 out of 100 cases, compared to 69 to 86 out of 100 with standard mammography[Evidence: A][2]
- Over a 10-year period, 3D mammography reduced unnecessary callbacks from about 11 out of 100 women to about 7 out of 100[Evidence: B][7]
- The American College of Radiology recommends 3D mammography for breast cancer screening in all women, regardless of risk level[Evidence: D][13]
Getting a mammogram can feel stressful, especially when you've heard about newer screening options and aren't sure which one is right for you. If you've been told you have dense breast tissue, or if you simply want the most thorough screening available, you've likely come across the term "3D mammography."
It's common to feel overwhelmed by the technical language around breast cancer screening. The good news is that the evidence behind 3D mammography is strong, and this guide breaks down everything you need to know in clear, practical terms.
In this article, you'll learn how 3D mammography works, how it compares to standard 2D mammograms, what the procedure actually feels like, and what your results mean. Whether you're scheduling your first mammogram or considering an upgrade, this guide is here to help.
❓ Quick Answers
What is 3D mammography (tomosynthesis)?
3D mammography, also called digital breast tomosynthesis (DBT), takes multiple X-ray images of your breast from different angles. A computer assembles these into thin 1-millimeter slices, allowing radiologists to examine breast tissue layer by layer. This reduces the tissue overlap that can hide cancers in standard 2D mammograms.
Is a 3D mammogram better than a regular mammogram?
Research shows 3D mammography detects about 16% more breast cancers than standard 2D mammography[Evidence: A][1]. It also reduces unnecessary callbacks by about 32%[Evidence: B][7], meaning fewer women experience the anxiety of being called back for additional imaging. Benefits are even more pronounced for women with dense breast tissue[Evidence: A][2].
Is 3D mammography painful?
Most women experience mild to moderate discomfort from breast compression rather than pain. Each compression lasts about 7 to 10 seconds per view, slightly longer than the 5 to 7 seconds for standard mammography. Taking 400 to 600mg of ibuprofen 45 to 60 minutes beforehand, and scheduling 7 to 10 days after your period starts, can significantly reduce discomfort.
How long does a 3D mammogram take?
The total appointment takes about 20 to 30 minutes, including check-in and changing. The active imaging portion takes 5 to 10 minutes. Each breast typically requires two views, with the X-ray arm sweep lasting about 7 seconds per view. The process is similar in length to a standard mammogram.
Does insurance cover a 3D mammogram?
Medicare fully covers 3D mammography as part of annual screening mammograms. Approximately 35 states have mandated private insurance coverage for 3D mammography. Medicaid coverage varies by state, with 43 or more states covering it as of 2025. For women without coverage, out-of-pocket costs typically range from $50 to $250 above the standard mammogram fee.
How much radiation does a 3D mammogram use?
A 3D mammogram delivers approximately 3 to 5 milligray (mGy) of radiation for both breasts, compared to about 1.5 to 2.0 mGy for a standard 2D mammogram. While roughly double the dose, it remains well within FDA-approved safety limits. Modern systems using synthetic 2D images eliminate the need for a separate 2D scan and can reduce total exposure[Evidence: B][3][Evidence: A][16].
Is 3D mammography safe for women with breast implants?
Yes, women with breast implants can safely undergo 3D mammography. The technologist uses a modified positioning technique called Eklund displacement, which gently pushes the implant back to image more breast tissue. Additional views may be needed. Discuss your implants with the imaging center when scheduling your appointment.
3D Mammography
Digital Breast Tomosynthesis (DBT) is a revolutionary imaging technology that allows doctors to see through layers of breast tissue with unprecedented clarity.
🔬 How Does 3D Mammography Work?
Think of standard 2D mammography as looking at a photograph of a stack of books piled on top of each other. You can see the covers, but the text on individual pages is hidden beneath layers. 3D mammography separates those "pages," allowing your radiologist to examine each thin layer of breast tissue individually.
Here is how the process works:
- Positioning: You stand at the mammography unit and your breast is placed on a flat support platform.
- Compression: A clear plastic paddle gently compresses your breast to spread the tissue evenly. This lasts about 7 to 10 seconds per image.
- Arc sweep: The X-ray tube moves in a slight arc (about 15 degrees) around your breast, capturing multiple low-dose images from different angles.
- 3D reconstruction: A computer assembles these images into a series of 1-millimeter-thick slices, creating a three-dimensional view of your breast tissue.
This slice-by-slice approach is what gives 3D mammography its clinical edge. Research shows that 3D mammography correctly detected breast cancer in about 88 out of 100 cases, compared to about 79 out of 100 with standard 2D mammography[Evidence: A][9]. The improvement comes from reducing the "masking effect," where overlapping normal tissue in a flat 2D image can hide small cancers.
The technology also significantly benefits women with dense breast tissue[Evidence: A][2]. Dense tissue appears white on mammograms, and cancers also appear white, making them harder to spot on 2D images. By viewing tissue layer by layer, 3D mammography helps radiologists distinguish between dense tissue and potential abnormalities.
Modern 3D mammography systems can also generate a synthetic 2D image from the 3D data, eliminating the need for a separate standard mammogram. Research confirms this approach is safe and fully preserves cancer detection performance[Evidence: A][16]. A systematic review found that adding 3D mammography to standard imaging detected about 2 to 3 additional breast cancers per 1,000 women screened[Evidence: A][10].
Now that you understand the technology, here is what the procedure actually feels like.
🧪 What to Expect: The Real User Experience
During the Procedure
You will stand at the mammography unit and position one breast at a time on a flat platform. The room is typically kept cool, around 65 to 68°F (18 to 20°C), for equipment calibration. You may feel cold in the hospital gown. A clear plastic paddle compresses your breast firmly. Most women describe this as a firm squeezing pressure rather than sharp pain.
The compression lasts about 7 to 10 seconds per view, and you will hear the quiet hum of the X-ray arm as it sweeps in a small arc around your breast. Unlike an MRI, there is no tunnel or enclosed space. You remain standing, and the machine moves around you. Each breast typically requires two views (top-to-bottom and angled), and the entire imaging process takes 5 to 10 minutes.
What You'll Feel After
There is no recovery time or activity restrictions. You can return to all normal activities immediately. Some women with fibrocystic breast tissue notice mild tenderness for 1 to 2 hours after compression, similar to post-exercise muscle soreness. Results are typically sent to your ordering physician within 1 to 7 business days, and some centers offer same-day reads.
If you receive a callback letter, try to stay calm. Approximately 85% of callbacks do not result in a cancer diagnosis. Most are benign findings that simply need additional imaging for clarity.
How to Make It Easier
- Schedule wisely: Book your appointment 7 to 10 days after your period starts, when breast tenderness is lowest.
- Take ibuprofen beforehand: 400 to 600mg of ibuprofen (Advil, Motrin) 45 to 60 minutes before the scan reduces compression discomfort.
- Skip deodorant and lotion: These products can appear as white spots on images and may require repeat imaging.
- Wear a two-piece outfit: You undress from the waist up, so a two-piece makes this faster and more comfortable.
- Practice deep breathing: Controlled breathing before compression reduces muscle tension, which can increase discomfort.
- Speak up: If compression is too painful, tell the technologist. It can be adjusted while still maintaining image quality.
- Bring prior mammograms: Comparison with previous images is one of the most effective tools for accurate reading and reduces callback rates.
📊 Screening Schedule and Guidelines
How often you should get a 3D mammogram depends on your age, risk factors, and the screening guidelines your healthcare provider follows. Two major organizations offer current recommendations.
The American College of Radiology (ACR) recommends mammography, including 3D mammography, for breast cancer screening in all risk categories[Evidence: D][13]. The ACR also recommends supplemental breast MRI screening for women at high risk[Evidence: D][13].
The US Preventive Services Task Force (USPSTF) recommends biennial (every two years) mammography screening for women aged 40 to 74[Evidence: D][14]. This is an expanded recommendation from the previous starting age of 50, giving more women access to earlier detection[Evidence: D][14].
| Population / Organization | Screening Recommendation | Frequency | Evidence |
|---|---|---|---|
| Women 40-74, average risk (USPSTF) | Mammography screening | Every 2 years | [D][14] |
| All risk categories (ACR) | Mammography including DBT | Annual | [D][13] |
| High-risk women (ACR) | Mammography + Breast MRI | Annual (both) | [D][13] |
| Women 75+ (USPSTF) | Insufficient evidence to recommend | Individual decision with doctor | [D][14] |
Important context: The USPSTF uses the general term "mammography" and does not specifically distinguish between 2D and 3D mammography[Evidence: D][14]. The ACR specifically recommends digital breast tomosynthesis (3D mammography) as the preferred screening method[Evidence: D][13].
For women with dense breast tissue, the USPSTF currently states there is insufficient evidence to recommend routine supplemental screening such as ultrasound or MRI[Evidence: D][14], while the ACR recommends additional screening for high-risk patients[Evidence: D][13]. Talk to your healthcare provider about which schedule is right for your individual risk factors, family history, and breast density category.
⚠️ Risks, Side Effects, and Warnings
The 3D mammogram is a quick, low-risk procedure. The most common concern is discomfort from breast compression, but this is brief and manageable. It's normal to feel anxious about medical tests, and understanding what to expect can help ease that worry.
Radiation Exposure
A bilateral 3D mammogram delivers approximately 3 to 5 mGy of radiation, roughly double the 1.5 to 2.0 mGy from a standard 2D mammogram. This is still well within FDA-approved safety limits and comparable to the natural background radiation you receive over a few months of everyday life. Modern systems that generate synthetic 2D images from the 3D scan can reduce total exposure by eliminating the need for a separate 2D mammogram[Evidence: B][3][Evidence: A][16]. The TOSYMA trial confirmed that safety profiles were similar between 3D and standard mammography groups[Evidence: B][15].
Compression Discomfort
Most women experience mild to moderate discomfort rather than pain during compression. Women with fibrocystic tissue or those who schedule close to their menstrual period may experience greater discomfort. Taking ibuprofen beforehand and scheduling during the least sensitive part of your cycle can help significantly.
Contraindications
Understanding the Dense Breast Limitation
While 3D mammography significantly improves cancer detection in women with dense breasts[Evidence: A][2], it does not solve the challenge entirely. In women with extremely dense breast tissue (BI-RADS Category D), sensitivity drops to about 39% with 3D mammography alone, compared to about 96% with abbreviated breast MRI[Evidence: B][8]. If you have extremely dense breasts and are at high risk, your doctor may recommend supplemental screening with breast MRI.
When to See a Doctor
Contact your healthcare provider if you notice any of these changes, regardless of your most recent mammogram results:
- A new lump or thickening in your breast or underarm area
- Changes in breast size, shape, or skin texture (dimpling, puckering)
- Nipple discharge, especially bloody discharge
- Persistent breast pain that does not go away
- Skin changes on the breast (redness, scaling, swelling)
It's common to worry that every change means something serious. Most breast changes are benign, but any new or unusual symptom should be evaluated promptly.
📋 How to Prepare for Your 3D Mammogram
Making the most of your 3D mammogram starts before you arrive at the imaging center. Here are practical steps to ensure a smooth experience.
Before Your Appointment
- Gather your records: Request copies of prior mammogram images, especially if switching imaging centers. Comparison with previous scans is one of the most valuable tools for accurate reading and can reduce your callback rate.
- Know your breast density: Under dense breast notification laws now in effect in all 50 US states, your mammogram report will include information about your breast density. Understanding your density category (A through D) helps you and your doctor decide if supplemental screening is needed.
- Check your insurance: Contact your insurance provider to confirm coverage for 3D mammography. Medicare covers it fully. If your state mandates coverage, your plan likely covers it with no additional cost.
Day-of Checklist
- Do not apply deodorant, antiperspirant, powder, or lotion to your underarm or breast area. These products can create white spots on images.
- Wear a two-piece outfit for easier changing.
- Bring your insurance card and photo ID.
- Arrive 15 minutes early for paperwork.
After Your Mammogram
- Results typically arrive within 1 to 7 business days.
- If you are called back, remember that approximately 85% of callbacks are benign findings requiring only additional imaging.
- Ask your provider to explain your BI-RADS category if it is included in your results.
Keeping Your Records
Keep a personal file of your mammogram reports and images. Many imaging centers now offer patient portals for digital access. Having your screening history in one place helps future radiologists compare images accurately, which is especially important if you move or change providers.
What to Look for When Choosing a 3D Mammography Provider
The quality of your screening results depends on the imaging facility and the radiologist interpreting your images. Here is what to consider.
Facility Quality Markers
- FDA certification (MQSA): All mammography facilities in the US must be certified under the Mammography Quality Standards Act (MQSA). Verify your facility's certification at fda.gov/mammography. Why it matters: Federal oversight ensures equipment quality and technologist training standards.
- ACR accreditation: Facilities accredited by the American College of Radiology meet additional quality standards beyond the federal minimum. Why it matters: ACR accreditation indicates higher proficiency testing and quality assurance.
- 3D mammography availability: As of March 2025, 92% of US mammography facilities have at least one DBT machine. However, not all machines at those facilities are DBT-capable. Confirm the specific machine when scheduling. Why it matters: Standard 2D-only machines cannot perform 3D imaging.
- Breast imaging specialists: Look for facilities staffed by fellowship-trained breast imaging radiologists. Why it matters: Subspecialty training improves diagnostic accuracy and reduces false positives.
Questions to Ask Your Provider
- Does this facility offer 3D mammography (tomosynthesis)?
- Is the radiologist who reads my images fellowship-trained in breast imaging?
- Will my results be compared with prior mammograms?
- What is the typical turnaround time for results?
- Will I be notified about my breast density category?
- What happens if my results are abnormal?
Red Flags
- No MQSA certification: Operating without federal certification is illegal in the US and indicates lack of quality oversight.
- No radiologist available for consultation: You should be able to discuss results with a qualified radiologist.
- Pressure to add unnecessary tests: Additional imaging should be based on clinical findings, not revenue generation.
- Outdated equipment: Ask when the mammography equipment was last upgraded. Current-generation DBT systems provide better image quality than older models.
How 3D Mammography Compares to 2D Mammography: What to Know
3D mammography (tomosynthesis) and standard 2D mammography both use X-rays to screen for breast cancer, but they differ in how images are captured and interpreted. Understanding these differences can help you make an informed choice about your screening.
| Feature | 3D Mammography (DBT) | Standard 2D Mammography |
|---|---|---|
| How It Works | X-ray arm sweeps in arc, creates 1mm slices | Single flat X-ray image per view |
| Cancer Detection Rate | 5.3 to 7.1 per 1,000 screened[Evidence: B][7][15] | 4.0 to 4.8 per 1,000 screened[Evidence: B][7][15] |
| Sensitivity | 86 to 88%[Evidence: A][1][9] | 79 to 80%[Evidence: A][1][9] |
| Callback (Recall) Rate | 3.0 to 7.2%[Evidence: B][3][7] | 3.6 to 10.6%[Evidence: B][3][7] |
| Dense Breast Performance | Significantly improved detection[Evidence: A][2] | Limited by tissue overlap |
| Radiation Dose (bilateral) | ~3 to 5 mGy (with synthetic 2D) | ~1.5 to 2.0 mGy |
| Compression Duration | 7 to 10 seconds per view | 5 to 7 seconds per view |
| US Facility Availability | 92% of mammography facilities (March 2025) | Universally available |
| Medicare Coverage | Fully covered | Fully covered |
Key takeaway: Over a 10-year period, 3D mammography detected about 54% more cancers than standard 2D mammography, while also reducing the proportion of advanced-stage cancers found at diagnosis from about 44% to about 33%[Evidence: B][7]. When a screening program switched from standard 2D to 3D mammography, it detected about 54% more cancers, roughly 2 additional cancers per 1,000 women screened[Evidence: C][11].
The TOSYMA trial, one of the largest randomized studies involving nearly 100,000 women, confirmed that 3D mammography with synthetic 2D was about 48% more likely to detect invasive breast cancer than standard 2D mammography (OR 1.48, p<0.0001)[Evidence: B][15]. A meta-analysis involving over 2.6 million patients confirmed that 3D mammography plus standard imaging detected invasive cancer in about 4 to 5 women per 1,000 screened[Evidence: A][5].
What About Breast MRI?
For women with extremely dense breast tissue (BI-RADS Category D), breast MRI is substantially more sensitive. One landmark study found breast MRI correctly detected cancer in about 96 out of 100 cases in this population, compared to about 39 out of 100 with 3D mammography alone[Evidence: B][8]. However, 3D mammography produced fewer false alarms, correctly clearing about 97 out of 100 women without cancer, compared to about 87 out of 100 with MRI[Evidence: B][8].
This means 3D mammography remains the preferred screening method for most women, while breast MRI may be recommended as a supplemental tool for those at highest risk or with extremely dense breast tissue[Evidence: D][13].
What The Evidence Shows (And Doesn't Show)
What Research Suggests
The clinical evidence supporting 3D mammography is extensive and consistent across multiple large studies. The overall strength of evidence is strong, based on 7 meta-analyses and 6 randomized or large comparative studies.
- A meta-analysis of 11 studies showed 3D mammography improved overall cancer detection by about 16% compared to standard 2D mammography (RR 1.16, 95% CI 1.02-1.31)[Evidence: A][1]
- Research involving over 2.6 million patients across 42 studies found that 3D mammography combined with standard imaging detected invasive breast cancer in about 4 to 5 women per 1,000 screened[Evidence: A][5]
- The TOSYMA trial involving nearly 100,000 women found 3D mammography was about 48% more likely to detect invasive breast cancer (OR 1.48, p<0.0001)[Evidence: B][15]
- Over a 10-year period with 272,938 screenings, 3D mammography detected 54% more cancers and reduced the proportion of advanced-stage cancers at diagnosis from 43.6% to 32.6%[Evidence: B][7]
- 3D mammography with synthetic 2D images performed equivalently to 3D plus a separate standard 2D scan, meaning the additional scan is unnecessary[Evidence: A][16]
What's NOT Yet Proven
- No randomized controlled trial has measured whether 3D mammography reduces breast cancer mortality. Current evidence uses improved detection rates as a surrogate endpoint. This is the most significant gap in the evidence base.
- Optimal screening frequency specifically for 3D mammography has not been established through dedicated comparative trials. Current frequency recommendations are based on standard mammography evidence.
- The clinical benefit of detecting additional early-stage cancers in women aged 75 and older remains uncertain[Evidence: B][6].
- The overall rate of cancers found between scheduled screenings was not significantly different between 3D and standard mammography (−2.92 per 10,000 screens, 95% CI: −6.39 to 0.54)[Evidence: A][4], though a more targeted geographic analysis showed a reduction of about 5.5 fewer per 10,000[Evidence: A][4].
- The USPSTF found insufficient evidence to recommend supplemental screening for women with dense breast tissue[Evidence: D][14].
Where Caution Is Needed
- In women with extremely dense breast tissue (BI-RADS Category D), 3D mammography sensitivity drops to about 39%, while breast MRI achieves about 96% sensitivity[Evidence: B][8]. Women in this category should discuss supplemental screening with their doctor.
- Radiation dose is approximately double that of standard 2D mammography (3 to 5 mGy vs 1.5 to 2.0 mGy bilateral). While within FDA-approved safe limits, this is a consideration for women undergoing frequent screening.
- 3D mammography cannot detect all breast cancers. No screening test has 100% sensitivity.
- Insurance coverage varies significantly by state and insurance plan. Confirm coverage before your appointment to avoid unexpected costs.
Should YOU Get This Test?
Best suited for: All women aged 40 and older undergoing routine breast cancer screening[Evidence: D][13][14]. Women with dense breast tissue (BI-RADS C or D) and those with elevated risk factors benefit most from the improved detection rates[Evidence: A][2].
Not recommended for: Women who are pregnant (defer until after delivery). Women with active breast infections should defer until treatment is complete.
Realistic timeline: Results are typically available within 1 to 7 business days. If called back, additional imaging is usually scheduled within 1 to 2 weeks. Approximately 85% of callbacks are benign.
When to consult a professional: Before your first mammogram, discuss your personal risk factors, family history, and breast density with your healthcare provider to determine the right screening schedule and whether supplemental imaging is appropriate.
Frequently Asked Questions
What does it mean to be called back after a mammogram?
A callback means your radiologist needs additional images or a different type of imaging to clarify something seen on your mammogram. This does not mean you have cancer. Approximately 85% of callbacks result in benign findings that require no treatment. Callbacks are more common on your first mammogram because the radiologist has no prior images for comparison. The additional imaging may include spot compression views, magnification views, or ultrasound. Studies suggest 3D mammography reduces callback rates from about 11 out of 100 to about 7 out of 100 women, meaning fewer women experience this stressful waiting period.
Is 3D mammography good for dense breasts?
Yes. 3D mammography significantly improves cancer detection in women with dense breast tissue. Research involving over 2 million women showed that cancer detection rates increased significantly when 3D mammography was used, with benefits observed across both moderately dense (BI-RADS C) and extremely dense (BI-RADS D) breast categories. In diagnostic settings, 3D mammography correctly identified cancer in 84 to 90 out of 100 cases in women with dense breasts, compared to 69 to 86 out of 100 with standard mammography. However, for women with the most extremely dense breasts, breast MRI remains substantially more sensitive.
What is the difference between 3D mammography and a breast MRI?
3D mammography uses low-dose X-rays, takes about 5 to 10 minutes of active imaging, and is the recommended screening tool for most women. Breast MRI uses magnetic fields (no radiation), takes 15 to 45 minutes, and is primarily recommended as supplemental screening for high-risk women. In women with extremely dense breast tissue, MRI detected cancer in about 96 out of 100 cases versus about 39 out of 100 with 3D mammography. However, 3D mammography has higher specificity (about 97% versus about 87%), meaning fewer false alarms. Your doctor may recommend one or both based on your individual risk profile.
How much does a 3D mammogram cost without insurance?
Without insurance, a 3D mammogram typically costs $50 to $250 more than a standard 2D mammogram. The total cost (including facility fee) often ranges from $200 to $500 depending on location and facility. Medicare fully covers 3D mammography as part of annual screening. Approximately 35 states mandate private insurance coverage, and 43 or more states cover it through Medicaid as of 2025. Check with your imaging center and insurance provider for exact costs before scheduling. Many facilities also offer financial assistance programs for uninsured patients.
How often should I get a 3D mammogram?
The ACR recommends annual mammography screening, including 3D mammography, for women in all risk categories. The USPSTF recommends biennial (every 2 years) screening for women aged 40 to 74. Your healthcare provider can help determine the best schedule based on your personal risk factors, family history, and breast density. Women at high risk may benefit from more frequent screening and supplemental imaging such as breast MRI.
Is 3D mammography safe during pregnancy?
Elective mammography screening, including 3D mammography, should be deferred until after delivery because it uses ionizing radiation. Radiation exposure during pregnancy carries potential risks to the developing fetus. If breast cancer is suspected during pregnancy, your doctor will discuss alternative imaging options, such as breast ultrasound, that do not involve radiation. After delivery, you can safely resume regular screening. If you discover you are pregnant shortly after a mammogram, talk to your doctor, but the radiation dose from a single mammogram is very low and unlikely to cause harm.
What is the BI-RADS score on my mammogram report?
BI-RADS (Breast Imaging Reporting and Data System) is a standardized scoring system developed by the American College of Radiology to communicate mammogram findings clearly. Category What It Means Typical Next Step 0 Additional imaging needed Callback for more images or ultrasound 1 Negative (no findings) Resume routine screening 2 Benign findings Resume routine screening 3 Probably benign Short-term follow-up (6 months) 4 Suspicious Biopsy usually recommended 5 Highly suggestive of cancer Biopsy strongly recommended 6 Known cancer Treatment planning Your report should also include your breast density classification (A through D). Ask your provider to explain both your BI-RADS category and density classification.
Can a 3D mammogram detect all types of breast cancer?
No screening test detects 100% of breast cancers. Research shows 3D mammography has a sensitivity of about 86 to 88%, meaning it correctly identifies cancer in about 86 to 88 out of 100 cases. Some cancers, particularly in extremely dense breast tissue, may still be missed. Emerging technologies like contrast-enhanced mammography (CEM) may further improve detection. One study found that adding CEM to 3D mammography detected about 7 additional cancers per 1,000 women with a personal history of breast cancer. Women with extremely dense breasts and high risk factors may benefit from supplemental screening with breast MRI.
How do I prepare for a 3D mammogram?
Preparation is straightforward. Do not apply deodorant, antiperspirant, powder, or lotion to your underarm or breast area on exam day, as these can appear as white spots on images. Wear a two-piece outfit for easier changing. If you have prior mammogram images from a different facility, bring them or have them transferred ahead of time. Consider scheduling 7 to 10 days after the start of your menstrual period when breast tenderness is lowest. If you are sensitive to breast compression, taking 400 to 600mg of ibuprofen 45 to 60 minutes before the appointment can help reduce discomfort.
Who should get a 3D mammogram?
The ACR recommends 3D mammography for breast cancer screening in all women, regardless of risk level. Women who may benefit most include those with dense breast tissue (BI-RADS C or D), women aged 40 and older, women with a personal or family history of breast cancer, and women with prior abnormal mammogram results. In women aged 67 to 74, 3D mammography detected more early-stage invasive breast cancers. The USPSTF recommends mammography screening beginning at age 40. Talk to your doctor about whether 3D mammography is right for your individual circumstances.
Our Accuracy Commitment and Editorial Principles
At Biochron, we take health information seriously. Every claim in this article is supported by peer-reviewed scientific evidence from reputable sources published in 2015 or later. We use a rigorous evidence-grading system to help you understand the strength of research behind each statement:
- [Evidence: A] = Systematic review or meta-analysis (strongest evidence)
- [Evidence: B] = Randomized controlled trial (RCT)
- [Evidence: C] = Cohort or case-control study
- [Evidence: D] = Expert opinion or clinical guideline
Our editorial team follows strict guidelines: we never exaggerate health claims, we clearly distinguish between correlation and causation, we update content regularly as new research emerges, and we transparently note when evidence is limited or conflicting. For our complete editorial standards, visit our Editorial Principles page.
This article is for informational purposes only and does not constitute medical advice. Always consult qualified healthcare professionals before making changes to your health regimen, especially if you have medical conditions or take medications.





References
- 1 . Impact of digital breast tomosynthesis on screening performance and interval cancer rates compared to digital mammography: A meta-analysis, PloS One, 2025, PubMed [Kanıt: A]
- 2 . Digital breast tomosynthesis for breast cancer screening and diagnosis in women with dense breasts - a systematic review and meta-analysis, BMC Cancer, 2018, PubMed [Kanıt: A]
- 3 . A randomized controlled trial of digital breast tomosynthesis versus digital mammography in population-based screening in Bergen: interim analysis (To-Be trial), European Radiology, 2019, PubMed [Kanıt: B]
- 4 . Interval breast cancer rates for tomosynthesis vs mammography population screening: a systematic review and meta-analysis of prospective studies, European Radiology, 2025, PubMed [Kanıt: A]
- 5 . Performance of Digital Breast Tomosynthesis, Synthetic Mammography, and Digital Mammography in Breast Cancer Screening: A Systematic Review and Meta-Analysis, Journal of the National Cancer Institute, 2021, PubMed [Kanıt: A]
- 6 . Comparative Effectiveness of Digital Breast Tomosynthesis and Mammography in Older Women, Journal of General Internal Medicine, 2022, PubMed [Kanıt: B]
- 7 . Breast Cancers Detected during a Decade of Screening with Digital Breast Tomosynthesis: Comparison with Digital Mammography, Radiology, 2024, PubMed [Kanıt: B]
- 8 . Comparison of Abbreviated Breast MRI vs Digital Breast Tomosynthesis for Breast Cancer Detection Among Women With Dense Breasts, JAMA, 2020, PubMed [Kanıt: B]
- 9 . Digital breast tomosynthesis for breast cancer detection: a diagnostic test accuracy systematic review and meta-analysis, European Radiology, 2020, PubMed [Kanıt: A]
- 10 . Systematic review of 3D mammography for breast cancer screening, Breast, 2016, PubMed [Kanıt: A]
- 11 . Increased Cancer Detection Rate and Variations in the Recall Rate Resulting from Implementation of 3D Digital Breast Tomosynthesis into a Population-based Screening Program, Radiology, 2016, PubMed [Kanıt: C]
- 12 . Addition of Contrast-enhanced Mammography to Tomosynthesis for Breast Cancer Detection in Women with a Personal History of Breast Cancer: Prospective TOCEM Trial Interim Analysis, Radiology, 2024, PubMed [Kanıt: B]
- 13 . ACR Appropriateness Criteria® Female Breast Cancer Screening: 2023 Update, Journal of the American College of Radiology, 2024, PubMed [Kanıt: D]
- 14 . Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement, JAMA, 2024, PubMed [Kanıt: D]
- 15 . Digital breast tomosynthesis plus synthesised mammography versus digital screening mammography for the detection of invasive breast cancer (TOSYMA): a multicentre, open-label, randomised, controlled, superiority trial, The Lancet Oncology, 2022, PubMed [Kanıt: B]
- 16 . Diagnostic performance of tomosynthesis plus synthetic mammography versus full-field digital mammography with or without tomosynthesis in breast cancer screening: A systematic review and meta-analysis, International Journal of Cancer, 2025, PubMed [Kanıt: A]
Medical Disclaimer
This content is for informational and educational purposes only. It is not intended to provide medical advice or to take the place of such advice or treatment from a personal physician. All readers are advised to consult their doctors or qualified health professionals regarding specific health questions and before making any changes to their health routine, including starting new supplements.
Neither Biochron nor the author takes responsibility for possible health consequences of any person reading or following the information in this educational content. All readers, especially those taking prescription medications, should consult their physicians before beginning any nutrition, supplement, or lifestyle program.
If you have a medical emergency, call your doctor or emergency services immediately.
